Fig. 44.1
Skin incisions planned for penile composite tissue harvesting
Fig. 44.2
View of the isolated dorsal penile vein (DPV), and dorsal penile nerves (DPN) on the milimetric scale under operating microscope (_8, Zeiss OP-MI, 6SD; Carl Zeiss, Goettingen, Germany)
Fig. 44.3
View of the isolated corpus spongiosum (CS) on the milimetric scale under operating microscope. CC corpus cavernosum, P preputium (_8, Zeiss OP-MI, 6SD; Carl Zeiss, Goettingen, Germany)

Fig. 44.4
The penile composite tissue ex vivo
Operative Technique for the Recipient
The penis of the recipient rat was rerouted through the scrotum to the outside instead of performing amputation, in order to reduce urinary tract infections and mortality of the recipient rat [6] by this maneuver, the preputial skin of the recipient rat was left as a hallow tube (Fig. 44.5). Next the saphenous artery, vein and the lateral femoral cutaneous nerve on the right side of the recipient rat were isolated and rerouted to the pubic region through a subcutaneous tunnel.
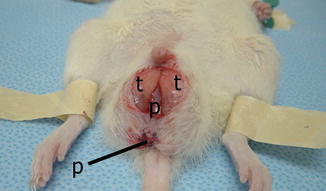
Fig. 44.5
View of the penis (p) that was rerouted to the most distal part of the scrotum passing through the testicle (t)
The neurovascular anastomoses between the penile composite tissue and the recipient were performed as follows: The corpus spongiosum of the graft was anastomosed directly to the saphenous artery and the dorsal vein of the graft was anastomosed to the saphenous vein of the recipient. Next the right dorsal penile nerve of the graft was coaptated to the right femoral cutaneous nerve of the recipient by using standard microsurgical techniques under operating microscope (×10 magnification) with 10/0 nylon sutures. Following completion of the neurovascular anastomoses, the transplanted penis was placed into the hollow tube formed by the preputial skin of the rerouted penis of the recipient. The preputial skin surrounding the glans of the graft was sutured to the distal part of the tube using 6/0 absorbable sutures. All the incisions were closed using 4/0 absorbable sutures at the end of the transplantation procedure (Figs. 44.6, 44.7 and 44.8).
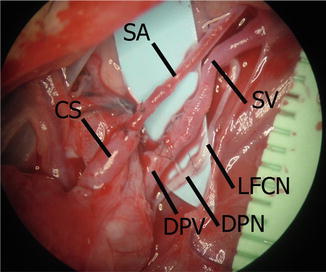
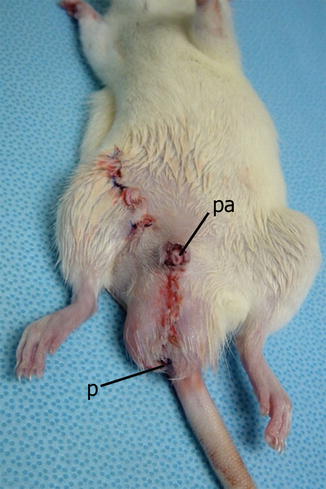
Fig. 44.6
View of the anastomoses on the milimetric scale under operating microscope. SA saphenous artery, CS corpus spongiosum, DPV dorsal penile vein, SV saphenous vein, DPN dorsal penile nerve, LFCN lateral femoral cutaneous nerve (_8, Zeiss OP-MI, 6SD; Carl Zeiss, Goettingen, Germany)
Fig. 44.7
Drawing of the design of the transplantation procedure
Fig. 44.8
View just after the operation. p penis, pa penis allotransplant
Evaluation of Viability of the Transplant
The transplants were evaluated clinically for viability and clinical signs of rejection on a daily basis for 100 days after the transplantation procedure. Somatosensory evoked potential analysis (SSEP) was performed at the 60th day post-transplant in order to evaluate sensory recovery of the transplant (Bio-Logic Systems Corp, Chicago, IL.). All the recipient rats were sacrificed at the 100th day after transplantation. Microangiographes were performed in order to visualize the vascularization of the transplants using the technique described elsewhere, followed by histological evaluation of the allografts [10].
Results
Anatomic Studies
The detailed anatomy of the penis of the rat was described before elsewhere [11–13]. Instead of following the main vascular branches proximally as described by Akyurek et al. [12] and Karamursel et al. [13], we have proved that the penis of the rat can be successfully arterialized by end-to-end anastomosis of the corpus spongiosum to the saphenous artery. The diameter of the dorsal penile vein (1.4 mm) was suitable for anastomosis to the saphenous vein (1.2 mm) for venous drainage of the transplant. The lateral femoral cutaneous nerve (0.7 mm) could be rerouted to the inguinal region after dissection and easily coaptated to the ipsilateral dorsal penile nerve (0.6 mm) for sensory recovery.
Isotransplantation
Related posts:
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
 Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Repair and Reconstruction of Defects After Resection of Chest Wall and Abdominal Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


