Abstract
In pediatrics, orbital fracture repair must be weighed against the potential skeletal growth disruption resulting from surgery and preventing globe malposition and motility complications. Pediatric orbital fractures are unique in presentation secondary to the evolving anatomy and physiology of the craniofacial skeleton. Therefore, the management of these fractures should be performed differently from adult patients. The understanding of these injuries is evolving and controversial in some aspects: particularly the decision to operate and the timing of the operation. For children with Type 1 orbital fractures, radiographic findings should not drive the decision to operate, independent of physical examination findings. A more conservative approach to operative management should be pursued when signs of muscle entrapment, acute enophthalmos, or hypoglobus are not present. The objective of this chapter is to highlight the pertinent differences in anatomy, presentation, and management, as well as clinical outcomes of pediatric orbital fractures.
Keywords
orbital trauma, pediatric orbital fracture, growing skull fracture, trapdoor fracture, white-eyed blow out, extraocular muscle entrapment, enophthalmos, diplopia
Background
Pediatric orbital fractures differ from the adult population in terms of presentation, management, and complications. The craniofacial skeleton undergoes significant anatomical and physiological changes from birth into adulthood; therefore, the fracture patterns in the pediatric population present differently, influencing diagnosis and management. The understanding of these injuries is evolving and controversial in some aspects: particularly the decision to operate and the timing of the operation. In pediatrics, fracture repair must be weighed against the potential skeletal growth disruption resulting from surgery versus preventing globe malposition and motility complications. The objective of this chapter is to highlight the pertinent differences in anatomy, presentation, and management, as well as clinical outcomes of pediatric orbital fractures.
Surgical Anatomy
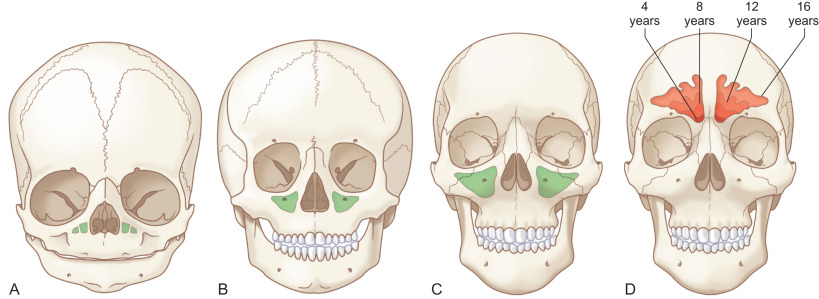
In the infant, the cranium is relatively large compared to the face, with an estimated ratio of 8 : 1. As the skeleton matures, facial growth predominates resulting in an adult cranium to facial ratio of 2.5 : 1. During major trauma, craniofacial fractures (i.e., orbital roof) are more likely than maxillofacial fractures (i.e., orbital floor) in early life due to a more prominent cranium and developing sinuses ( Fig. 2.3.1 ).
Seven bones articulate to form the orbit: frontal, maxillary, zygomatic, palatine, ethmoid, lacrimal, and sphenoid. Three of the four orbital walls – roof, floor, and medial wall – are adjacent to a sinus. In the setting of trauma, the sinuses help dissipate the force transmitted to the facial skeleton and brain.
The sinuses begin to separate from the nasal cavity in utero, and begin to pneumatize and expand after birth. The maxillary sinuses are the first to develop, but in a biphasic pattern, with a delay between 7 and 12 years of age. During this period of mixed dentition, the cuspid teeth are unerupted in the maxilla, directly below the orbital floor. The halt in pneumatization results in increased bone stock beneath the orbital floor, helping the floor resist fracture. As the permanent dentition erupts, maxillary sinus growth continues, reaching adult size by age 16.
The ethmoid sinuses grow from birth to age 12, from anterior to posterior. As they expand, the medial orbital wall becomes progressively thinner and more susceptible to fracture. At adulthood, the medial wall is named the lamina papyracea or “paper wall.”
The frontal sinuses pneumatize and enlarge, typically starting at age 7, completing growth in adulthood. Prior to their development, traumatic forces placed on the superior orbital rim are not dissipated through the frontal sinus but rather, transmitted to the roof, causing either roof fractures or cranial fractures extending into the orbit. Posnick et al. reported a relatively high incidence of pediatric orbital roof fractures, representing 18% of orbital fractures in their cohort. Losee et al. reported an even higher incidence, at 33.3%. Lastly, orbital floor fractures become more common than orbital roof fractures with increasing age, following the timeline of maxillary sinus pneumatization.
There are also physiological differences in the craniofacial tissues that help the pediatric skeleton resist fracture. Pediatric bones have a higher proportion of cancellous bone, which has less stiffness than cortical bone. The stiffness of a material is inversely related to its elasticity – the material’s ability to deform with force. Cancellous bone can therefore better conform to traumatic forces, resulting in higher incidence of “greenstick” fractures or minimal to no displacement. The metabolic turnover of the pediatric skeleton is also significantly greater. Clinically, this means that the healing and remodelling potential of the pediatric skeleton is superior, supporting nonoperative management.
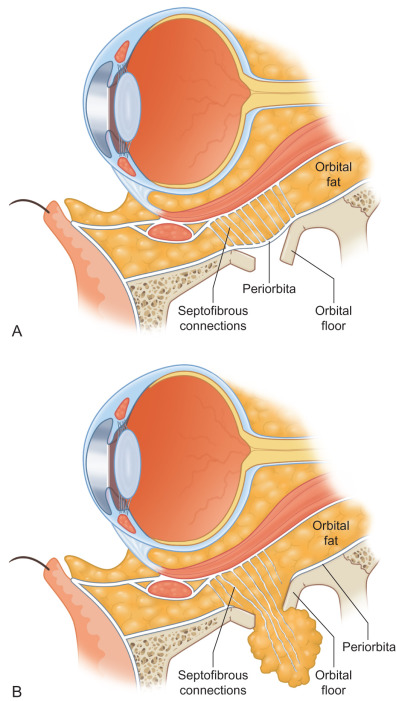
Increased elasticity of the periorbital soft tissue also helps avoid operative management in many cases. The periosteal lining, supporting check ligaments, and suspensory ligaments of the orbital cavity, can also help resist deformation, even in the setting of fracture. The elastic soft tissue may act to splint fractures or, in the setting of a blow-out fracture, prevent orbital malposition ( Fig. 2.3.2 ). Increased skeletal elasticity also means that a more significant amount of force is required to cause pediatric fractures. This, in addition to rudimentary sinuses, leads to more transmitted force to the neurocranium. Losee et al. found that 43.4% of pediatric orbital fractures were associated with neurosurgical injuries.
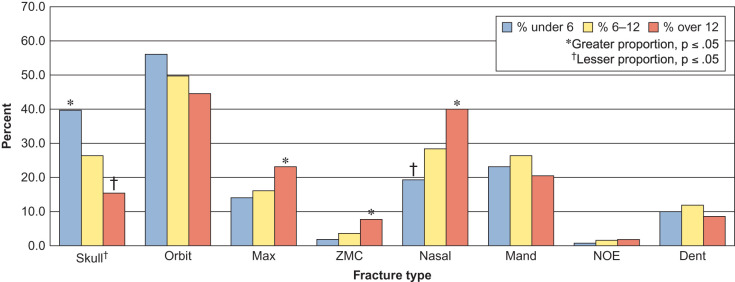
Pediatric facial fractures are relatively uncommon due to the aforementioned bone elasticity, cancellous composition, and higher cranium-to-face ratio. Within pediatric facial fractures, orbital fractures have a wide reported incidence, ranging from 3% to 45% of all facial fractures. Grunwaldt et al. demonstrated that the orbital fracture was the most common facial fracture ( Fig. 2.3.3 ) in all age groups (0–5 years, 6–12 years, 13–18 years). This differs from prior work evaluating the epidemiology of pediatric facial fractures. However, Grunwaldt et al. utilized emergency department-based assessment at a level one trauma children’s hospital, eliminating an inherent selection bias of individual surgeons, consulting department, and hospital admissions.
Classification
Orbital fractures can be isolated to the orbital walls or they can extend into adjacent structures. To guide management based on the presenting pattern, Losee et al. described a pediatric orbital fracture classification system based on three presenting patterns: pure orbital fractures, craniofacial fractures, and orbital fractures associated with common fracture patterns ( Table 2.3.1 ).
| Type 1 | Pure orbital fractures |
| 1a | Floor fractures |
| 1b | Medial wall fractures |
| 1c | Roof fractures |
| 1d | Lateral wall fractures |
| 1e | Combined floor and medial wall fractures |
| Type 2 | Craniofacial fractures |
| 2a | Growing skull fractures |
| Type 3 | Orbital fractures associated with common fracture patterns |
| 3a | Fractures of the floor and inferior orbital rim |
| 3b | Zygomaticomaxillary fractures |
| 3c | Naso-orbito-ethmoid fractures |
| 3d | Other fracture patterns |
Pure orbital fractures (Type 1) describe fractures limited to the orbit without extension into adjacent structures, and can be subdivided into five subcategories: floor, medial wall, combined medial wall and floor, superior roof, and lateral wall. Type 1 fractures are commonly referred to as “blow-out” or “blow-in” fractures but without involvement of the orbital rim. The orbital floor is the most common wall involved.
Craniofacial fractures (Type 2) describe fractures of the skull that extend into the orbital roof. This type of fracture is commonly seen in younger pediatric patients, often with neurological injury. The orientation also tends to be obliquely positioned, traveling from the frontal bone or temporal bone crossing diagonally through the orbital roof and extending to the orbital apex or sphenoid wings. Growing skull fractures are a unique complication of Type 2 fractures, which involve bony and dural disruption in the setting of surface tension on the dura, which most commonly arises from the growing brain. As the dural and bony defects enlarge, there is herniation of the leptomeninges, causing pulsatile proptosis, vertical orbital dystopia, and perhaps vision loss.
Common pattern fractures (Type 3) are orbital fractures that occur in the setting of a well-described facial fracture pattern. This group can be further separated into four subcategories: impure blow-out fractures involving the orbital rim, zygomaticomaxillary complex fractures, naso-orbito-ethmoid fractures, and other fracture patterns such as Le Fort II and III fractures. The orbital fractures in this group tend to be more displaced, and the associated fractures often carry indications for operative management.
Clinical Presentation
Obtaining an adequate history and physical examination in the pediatric patient can be difficult due to the uncooperative nature of this patient population. Furthermore, the clinical presentation of orbital fractures in children is often different from the adult due to many of the anatomical and physiological differences described earlier. Therefore, there should be a low threshold for obtaining radiographic imaging when neurological injury or fracture is suspected.
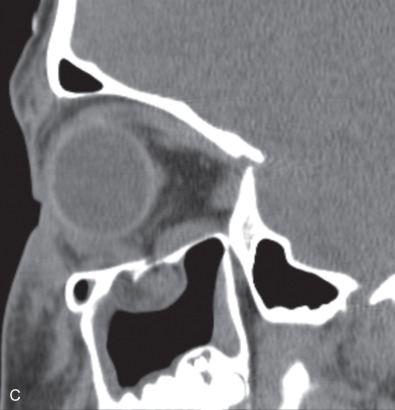
While comminuted “blow-out” fractures are commonly seen in adults, linear, minimally displaced fractures occur more commonly in the pediatric orbit. The elasticity of the pediatric orbital bone is the key difference, resulting in a unique clinical presentation: trapdoor fractures. The trapdoor pattern describes the entrapment of orbital tissue, the most concerning of which are extraocular muscles, in a linear orbital wall fracture that is usually minimally or non-displaced ( Fig. 2.3.4 ). When force is placed on the orbit, the intraorbital pressure increases and creates a fracture of the orbital wall. Periorbital tissue is then pushed into the open fracture. In the adult, the fracture remains open and displaced, resulting in the classic “blow-out” presentation characterized by enophthalmos and/or hypoglobus. In the pediatric patient, however, the bone fracture is incomplete, and the partially fractured bone will rapidly recoil back to the original position trapping the periorbital tissue and leading to possible strangulation. Furthermore, children presenting with radiographic “blow out” fractures often times do not present with globe malposition as do their adult counterparts ( Fig. 2.3.5 ). The periosteum and supporting soft tissue may remain intact, maintaining orbital volume despite a large displaced wall fracture.





Subconjunctival hemorrhage in the setting of orbital trauma is always a sign of possible orbital fracture. However, the absence of this finding in the pediatric patient does not rule out a diagnosis of an entrapped orbital wall fracture. This presentation was termed “white-eyed blow-out” fracture by Jordan et al. in 1998. The conjunctiva may appear normal, but the entrapped periorbital tissue will result in severe gaze restriction. Radiographically, a fracture may not be significantly displaced, but periorbital tissue may often be identified in the adjacent sinus.
Entrapment of the extraocular muscles can result in the oculocardiac reflex, describing the clinical constellation of bradycardia, nausea, and syncope. Aschner first described this phenomenon in 1908 with a decrease in heart rate when applying pressure to the globe. In addition to muscle entrapment, other triggering stimuli including ocular pain, increased intraocular pressure, and globe injury. Patients demonstrating signs of the oculocardiac reflex need urgent treatment, ophthalmic consultation, and forced duction assessment.
Given the elasticity and the robust nature of the pediatric facial skeleton and soft-tissue, higher traumatic forces are needed to cause facial fractures. Therefore, pediatric patients with facial fractures frequently have other associated injuries. Losee et al. found that 60% of children presenting with an orbital fracture had a nonfacial laceration, 12.6% had an ocular injury, 43.4% had a neurosurgical injury, and 20% had a significant injury beyond their head and neck. Pediatric facial fractures with more severe injuries to the regions of the head and chest are associated with a higher mortality. The high incidence of associated injuries in pediatric orbital fractures reinforces the importance of a thorough primary and secondary traumatic survey and a multidisciplinary approach to assessment and management.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


