Abstract
This chapter addresses pediatric fractures of the mandible. It elaborates on the epidemiology, relevant anatomy, treatment options, and complications.
Keywords
pediatric, mandible, fracture, dental, ankylosis, complications, conservative
Background
The topic of pediatric mandible fractures covers a wide range of patients with multiple clinical variables. Patients can range from a neonate with a mandible fracture stemming from birth trauma to an 18-year-old with full permanent dentition and multiple fractures. Because of this range of differences, the “pediatric” population in regards to mandible fractures can be further divided into the following:
Neonate/infants – 0 to 1 year of age (developing/unerupted dentition)
Toddlers – 1 to 3 years of age (erupting primary dentition)
Children – 4 to 12 years of age (primary and mixed dentition)
Adolescents – 12 to 18 years of age
The incidence of pediatric mandible fractures, as demonstrated in Imahara’s review of the National Trauma Data Bank from 2001 to 2005, is not insignificant. Imahara found that of 12,739 pediatric patients diagnosed with facial fractures, the most common fracture was that of the mandible (32.7%). A recent review of the Healthcare Cost and Utilization Project’s National Emergency Department Sample demonstrated mandible fractures (defined as fractures in patients 18 years of age and younger) to have a 4 : 1 male to female ratio and an overall mean age of 14 years. The major etiologies of mandible fractures in this study included falls (17%), motor vehicle collisions (13%), and assault (8%). The mechanism of trauma varies according to age, with the leading cause in both females and males in patients under 12 years of age being falls, while male and older adolescent (≥12 years) patient populations had assault as their leading cause of mandible fracture.
The site of fracture also varies according to age. Owusu and colleagues reviewed more than 1200 mandible fractures in pediatric patients, revealing that the most commonly fractured anatomic sites of the mandible varied depending on age. This is likely a result of two factors: first, the developing dentition, which would provoke changes in the mandible’s weak points as teeth develop and erupt, and second, the change in the mechanisms based on the common activities specific to each age group. Young patients (≤12 years of age) most commonly fractured the condyle (27.9%) while older patients’ most common site of fracture was the angle (17.6%). Several additional studies have demonstrated that while many pediatric mandibular condylar fractures will occur in isolation, up to 20% will present with bilateral condylar fractures. Mandible fractures also occur with concomitant injuries in regions other than the face in 11%–65% of trauma patients. Forces that are significant to fracture a pediatric mandible have a high likelihood of concomitant injury. Injuries associated with mandible fractures include other facial fractures (13%), facial soft tissue injury (34%), C-spine (0.9%–4.4%), neurocranial (8.5%–34%), extremity (9.1%–16.4%), chest (1.8%), and abdominal injuries (1.6%). Concomitant injuries vary based on the mechanism of injury. While ER visits involving facial fractures are relatively uncommon (0.03%), all surgeons are mandatory reporters of suspected child abuse—any suspicion of the mechanism/injury should provoke notification through the proper channels for investigation and any necessary intervention.
Embryology and Growth of the Mandible
The mandible develops by intramembranous ossification and is derived from the first branchial cleft with contributions from the proximal portion of Meckel’s cartilage. By the sixth week of embryologic development, the bilateral mandibular processes have fused to form a fibrous symphysis. The mandible is then the second site (after the clavicle) to undergo ossification. Ossification continues throughout the first year of life.
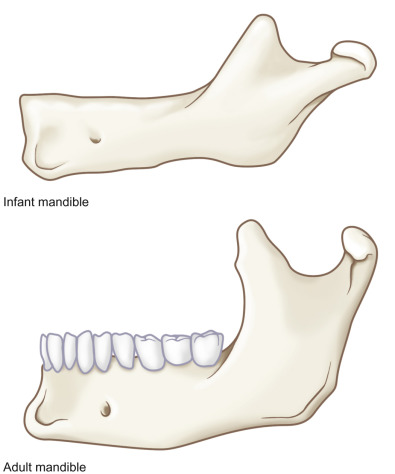
The growth of the mandible is a complex, multifactorial process. Its growth is influenced by the growth of the alveolar process, the developing dentition, the associated muscular processes, and the mandibular condyle. Disruptions in growth (either due to congenital factors or due to trauma) can lead to abnormal development, with significant cosmetic and functional consequences, including asymmetries and malocclusions ( Fig. 2.5.1 ).
The importance of the relationship of the developing dentition to alveolar growth cannot be overstressed. In patients with congenitally missing dentition (such as ectodermal dysplasia), the alveolar process is undeveloped. The growth of the alveolar process mirrors the eruption sequence. After tooth eruption, the mechanical forces of mastication and parafunctional habits exert forces on the alveolar bone that will also influence development and maintenance of bone. While this complex process has not been fully elucidated, it is imperative that the surgeon understands the interactive role the developing dentition plays in alveolar bone development and does everything possible to minimize disruption during the treatment of mandible fractures.
The position of the mental foramen changes relative to the mandibular body throughout mandibular growth. At age 3 it lies between the deciduous canine and first molar and is near the inferior border. By age 6, the mental foramen is posterior and superior in its relative position, eventually residing inferior to the first or second premolar and is no longer near the inferior border, but is often equidistant between the inferior and superior aspect of the mandibular body.
The muscles of mastication play a role in the development of both the coronoid process and mandibular angle (which grow by periosteal apposition). However, disruption of these regions with fractures rarely impacts the overall growth of the mandible.
The mandibular growth derived from the condylar process is complex and fracture of this region can impede growth and result in asymmetry and malocclusion. While other growth mechanisms exist within the mandible, the condyle is a major contributing source of both vertical and horizontal growth of the mandible. The growth of the condylar process is linked to the presence of secondary cartilage in this location. The direction of this growth of the condyle is influenced by the mandibular posture, condyle/fossa relationship, and a multitude of mechanical factors. Fractures of the condyle can have a significant impact on normal mandibular growth/development and will be discussed later in this chapter.
Anatomy of the Mandible
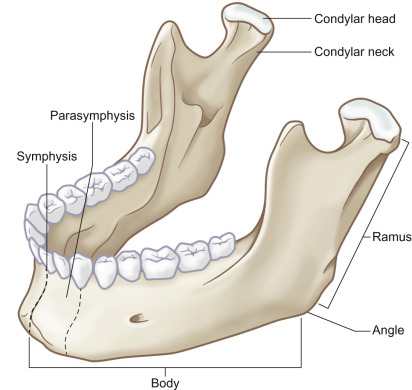
The bony mandible is comprised of the following anatomic subunits: the condyle, condylar neck, ramus, angle, body, and symphysis. Use of these terms in describing the injury is paramount in helping a practitioner understand the problem at hand – as fractures of the mandible are treated differently based on the age of the patient and the anatomic subunit involved ( Fig. 2.5.2 ).
The third division of the trigeminal nerve (cranial nerve V) provides sensory innervation to the mandible after exiting the foramen ovale. This nerve also provides innervation to the muscles of mastication (masseter, temporalis, and medial/lateral pterygoid muscles). The major arterial supply to the mandible is the inferior alveolar artery (a branch of the internal maxillary artery). The associated inferior alveolar vein completes the neurovascular bundle that enters at the mandibular foramen proximally and divides at the first molar region into an incisive branch that continues anteriorly within the mandible and a mental branch that exits at the mental foramen. The orientation of the neurovascular bundle is that the vein (or veins) reside superior to the nerve, and the artery is located lingual to the nerve.
The mandible is a bone suspended in space by its musculature. The paired muscles that help with mastication are the medial and lateral pterygoids, masseter, temporalis, with some contribution from the digastric muscles. The medial aspect of the mandibular body is the site of attachment for the mylohyoid and the anterior lingual aspect provides the site of attachment for the digastric, the genioglossus, and geniohyoid muscles. The mandible is also the site of attachment for the paired muscles of the mentalis (anteriorly) and buccinator (superiorly at the posterior body), as well as the platysma (along the inferior border).
This complex musculoskeletal unit provides the ability for basic life functions such as speech and mastication. An injury to the mandible can lead to compromise, and its proper repair is necessary in reestablishing both form and function.
Stages of Dentition
Understanding the dentition and its stages is crucial in the treatment of pediatric mandible fractures. In general, pediatric mandible fractures can be divided into three simple groups: primary dentition, mixed dentition, and permanent dentition stages. The dentition phase, as well as the condition of the dentition, will significantly affect the treatment plan for mandible fractures.
The tooth buds for the primary teeth are present in utero with the dental lamina from which they develop present as early as 12 weeks in utero. The first teeth to erupt are most often the lower central incisors at 6–10 months of age. The primary dentition is comprised of 20 teeth that most often erupt prior to age 3 ( Fig. 2.5.3 ). Primary teeth have crowns that are more bulbous than their permanent counterparts, and have roots with increased divergence, which allows space for the development of permanent tooth buds inferiorly. The roots of primary teeth will resorb as the permanent teeth develop and begin to erupt, ending with the exfoliation of the primary teeth. Primary teeth should have some spacing between all of the teeth, although spacing between the primary teeth will close with the eruption of the first permanent molar, which ushers in the beginning of the mixed dentition phase.

The mixed dentition phase begins around age 6 and extends until approximately age 12 when the final primary tooth exfoliates ( Fig. 2.5.4 ). The mixed dentition presents significant challenges in establishing the maxillomandibular relationship due to unerupted or partially erupted permanent teeth, loose deciduous teeth that have not exfoliated, and discrepancy in crown size of the newly erupted permanent dentition adjacent to smaller, retained primary teeth. These challenges can impede the placement of secure maxillomandibular fixation (MMF) for both closed and open procedures to correct alignment of a mandible fracture. Similarly to the primary dentition phase, existing unerupted tooth buds within the mandible can present challenges when open reduction/rigid fixation is required.

Following the exfoliation of the final primary tooth, the dentition is considered to be in the permanent dentition phase ( Fig. 2.5.5 ). It is at this point that the methods of treatment for a mandible fracture begin to mirror the treatments rendered in the adult population. The fracture patterns of the mandible also resemble that of the adult population.
Fracture Patterns in Pediatric Populations
Fracture patterns in pediatric populations vary based on the stage of the dentition of the patient as both the activities a child/youth/adolescent is involved in and the weak points of the mandible vary with age. In various studies evaluating the distribution of mandible fractures in pediatric patients, the condylar (condylar neck or condylar head) region is consistently the most frequently fractured structure (7%–45%), the parasymphysis is the second most frequently injured (20%–32%), the percentage of angle fractures ranges from 4.4% to 45%, with an increased incidence during the teenage years, coinciding with third molar development. Siegel et al. demonstrated that children in mixed dentition aged 7–12 have increased risk of mandibular body fractures (20%) compared to younger children aged birth to 6 (4.4%) or those aged 13–18 years (9.7%). Patients often presented with multiple fractures (28%–59%).
Evaluation
Evaluation of the mandible during the secondary trauma survey (following ATLS protocol) should replicate the exam in an adult patient – however, it will often require patience and ingenuity. A thorough evaluation of the mandible will include examination of the temporomandibular joints, bony continuity at the posterior/inferior border, dentition, occlusion, and the associated soft tissue.
The temporomandibular joint (TMJ) should be assessed for appropriate range of motion, tenderness overlying the joint, pop/click/crepitus, and deviation on opening. From the TMJ region, the practitioner should palpate for bony steps or irregular surface along the posterior border of the ramus and inferior border of the body and symphysis region, also noting any discrete regions of tenderness. The dentition should be inspected for loose or missing teeth as well as “steps” in the occlusal plane. The occlusion with the maxillary dentition (if intact) should be evaluated for a stable/repeatable occlusion, as alterations in occlusion can be indicative of fracture or TMJ hemarthrosis/edema. The overlying attached and unattached gingival tissues require inspection for lacerations and bleeding, which often harbor fragments of traumatized dentition (or entire teeth).
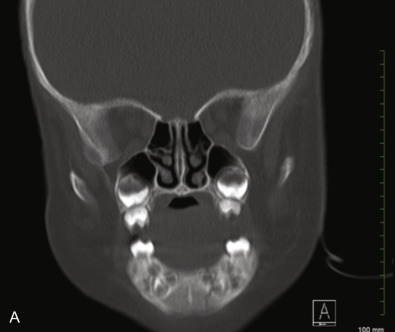
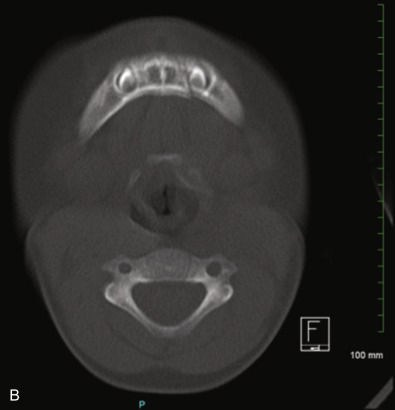
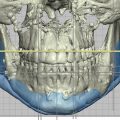
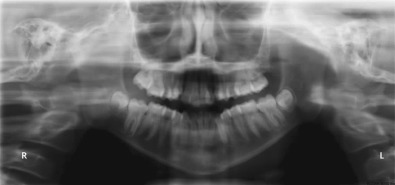
Imaging of the mandible for suspected fractures/injury is best performed with a combination of images. Imaging of the mandible can be accomplished with a single panoramic image ( Fig. 2.5.6 ). This single image allows visualization of the mandible and dentition in its entirety on a single image with minimal radiation exposure. Unfortunately, young patients may not be tall enough or remain motionless long enough for this image to be obtained, and many emergency rooms and trauma centers are not equipped to provide this image as it is most often employed in a dental setting. AP and lateral mandible films can be helpful in augmenting the panoramic image ( Fig. 2.5.7 ). They may be used alone to demonstrate fractures, but can be difficult to interpret if the practitioner is not accustomed to viewing these images and non-displaced fractures or greenstick fractures (more common in pediatric populations) can be missed. For all of the above reasons, further characterization of mandible fractures is most often provided by a non-contrast computerized tomogram (CT) of the mandible ( Fig. 2.5.8 ). Appropriate imaging ensures extension of the area imaged from the glenoid fossa to the inferior border of the mandible. Finally, surgeons who have cone beam technology available to them can utilize this method of imaging to decrease radiation dose, while still affording axial, coronal and sagittal slices for three-dimensional evaluation of the injury, but like a panoramic image they require a patient to remain motionless in an upright position for the period of time it takes to obtain the image.