Dermoscopic analysis of pigmented skin lesions is based on four algorithms:
- •
pattern analysis;
- •
the ABCD rule;
- •
Menzies’ 11-point checklist; and
- •
the 7-point checklist.
The common denominator of all these diagnostic algorithms is the identification and analysis of dermoscopic criteria found in the lesions. The majority of the dermatologists who participated in the second consensus meeting were proponents of pattern analysis. The basic principle is that pigmented skin lesions are characterized by global patterns and combinations of local criteria.
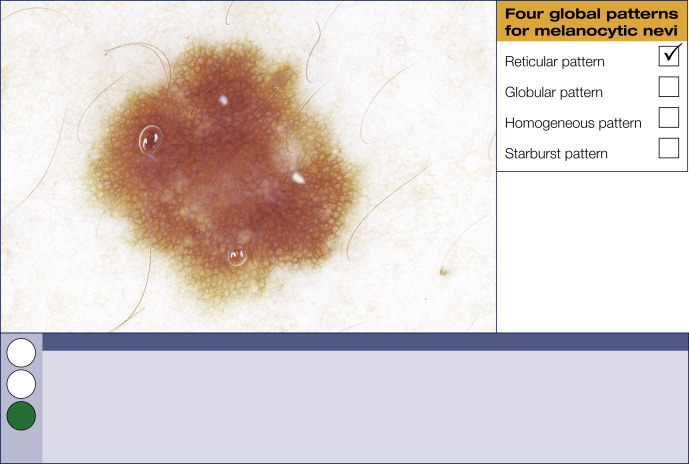
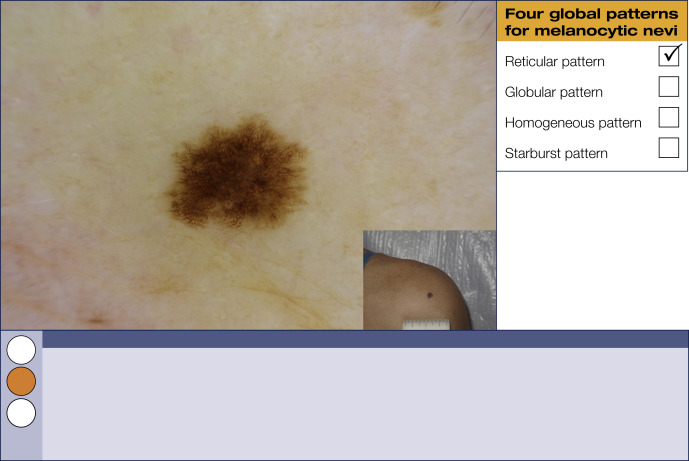
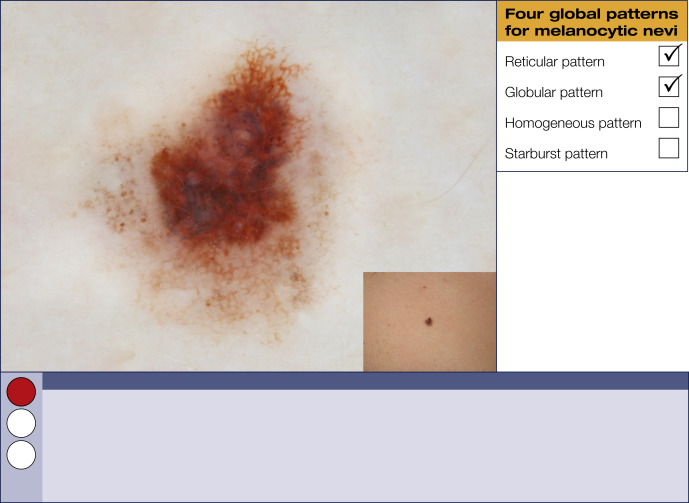
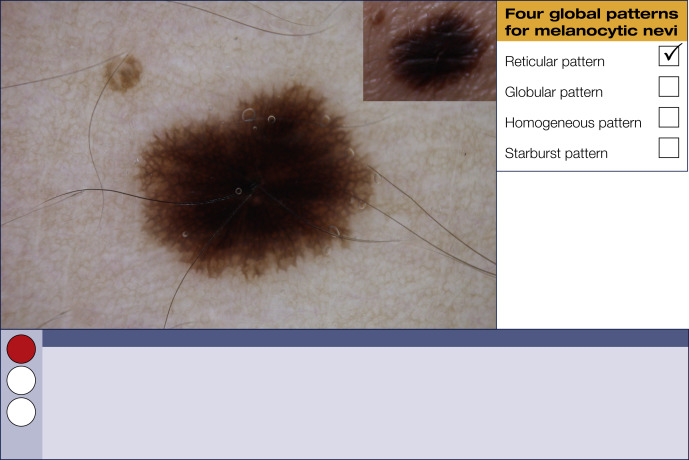
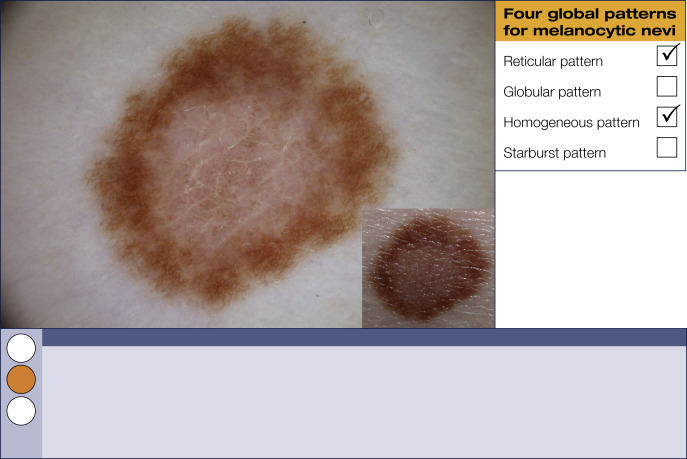
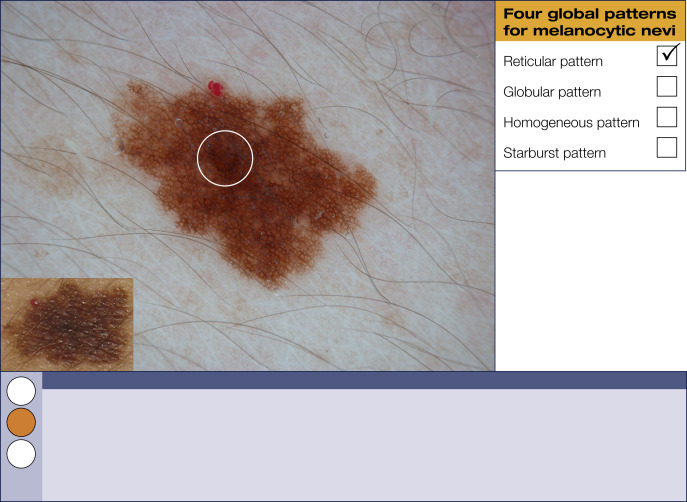
Four global dermoscopic patterns for melanocytic nevi
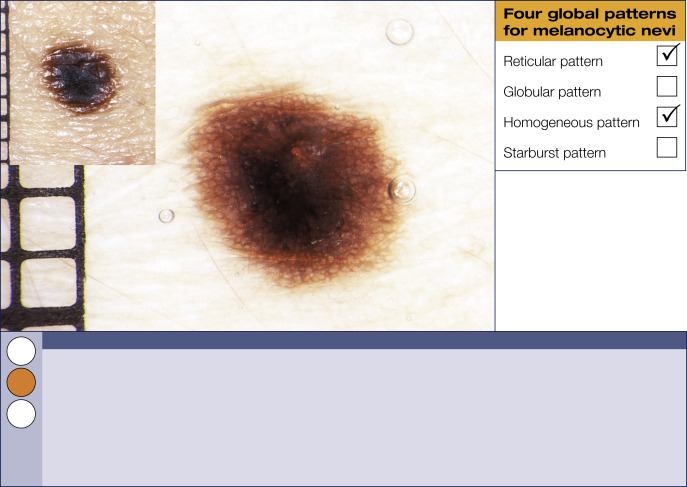
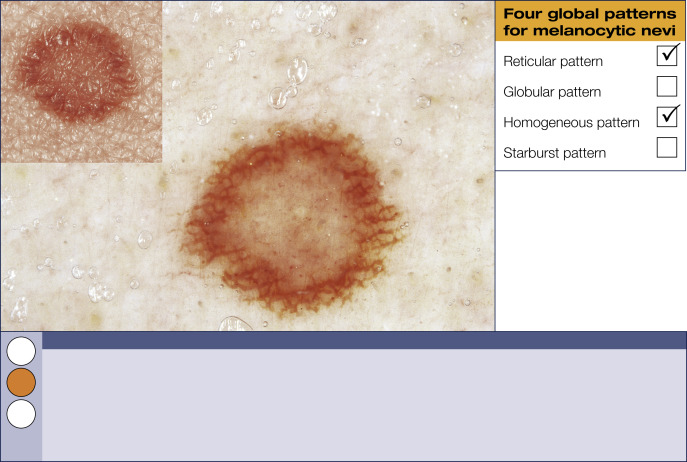
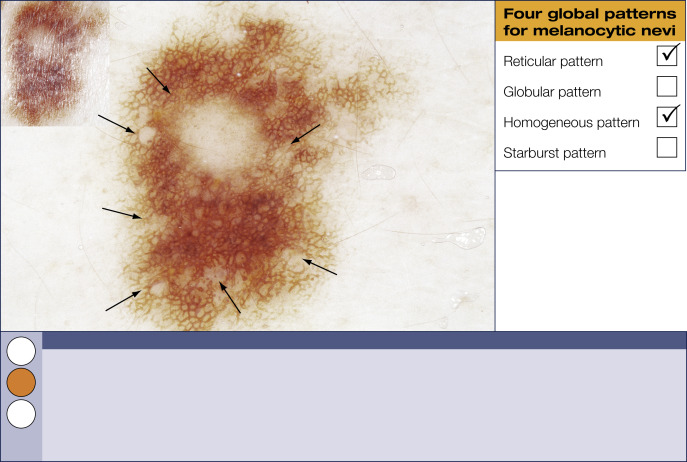
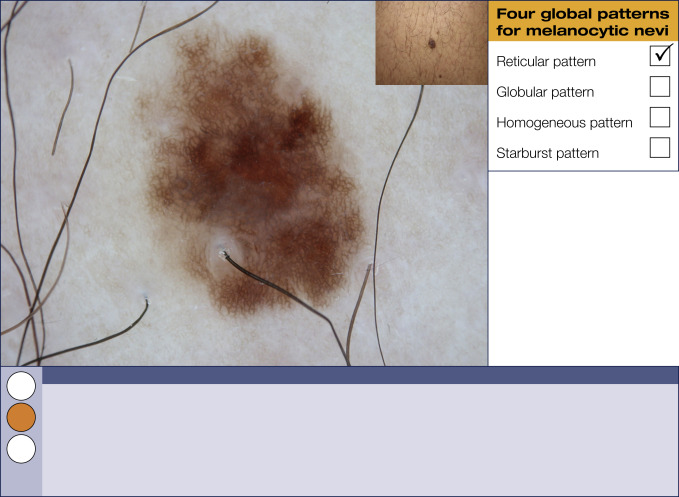
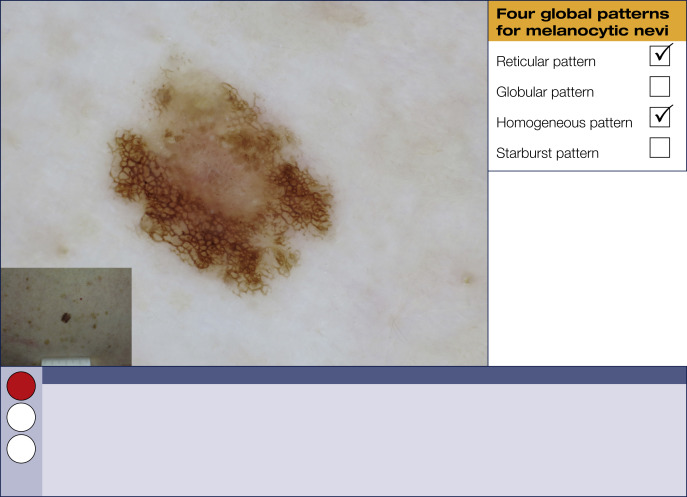
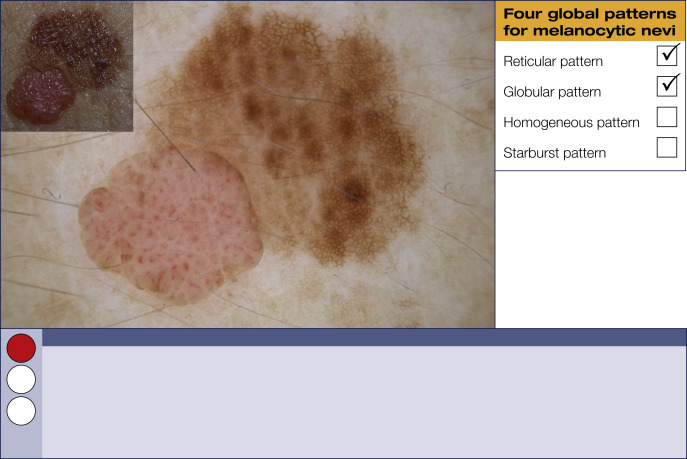
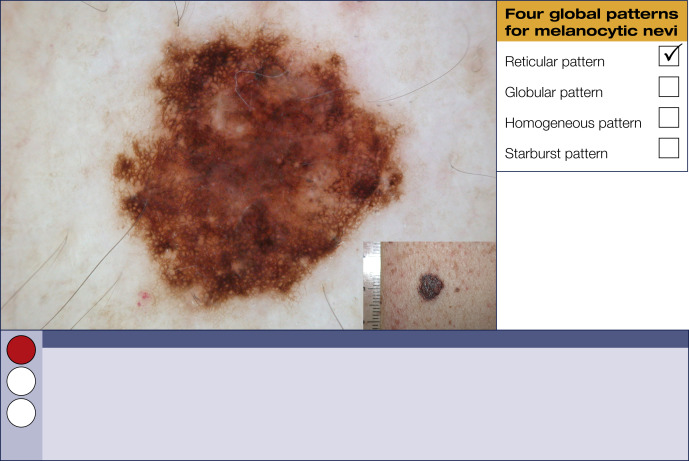
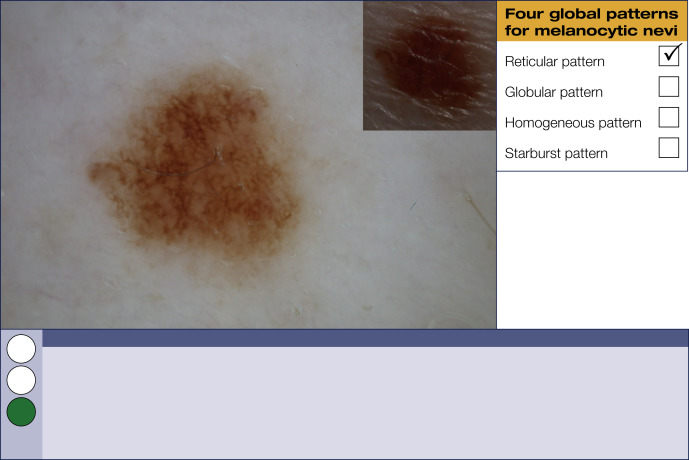
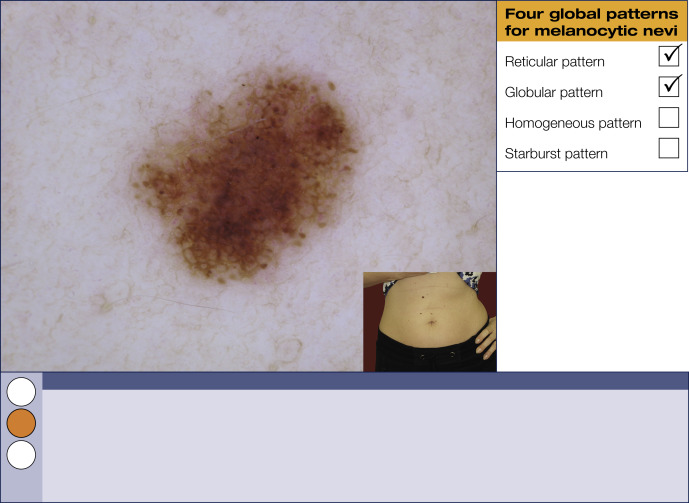
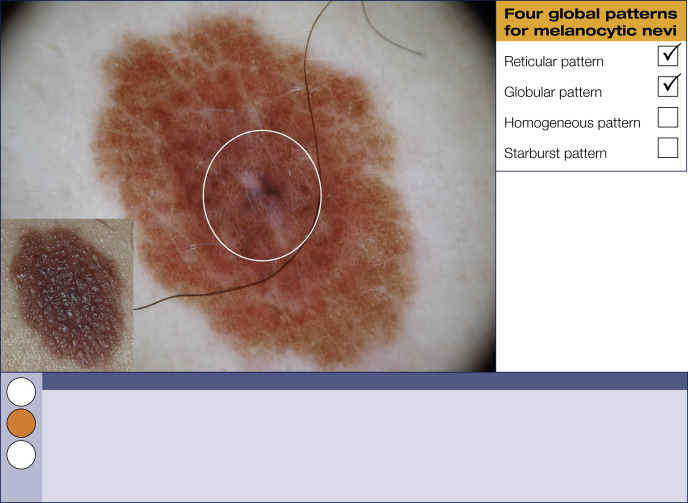
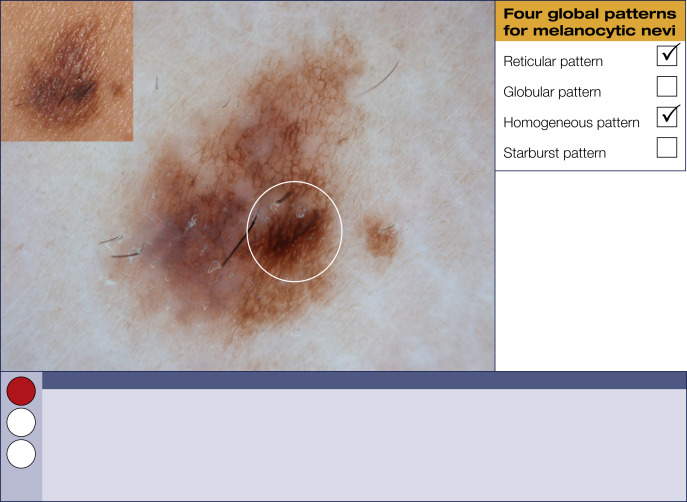
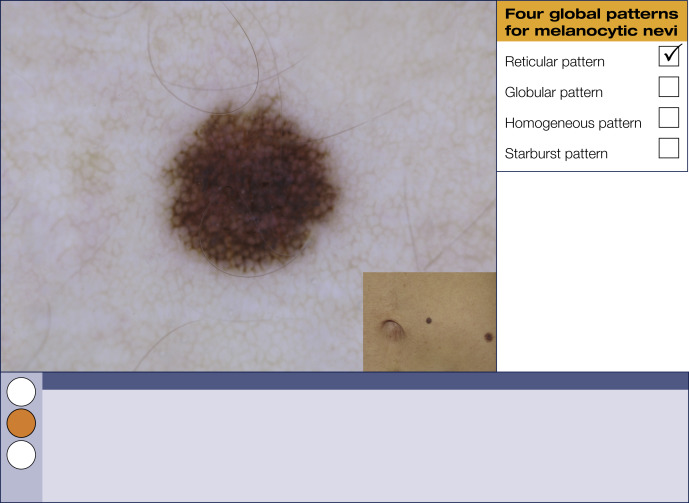
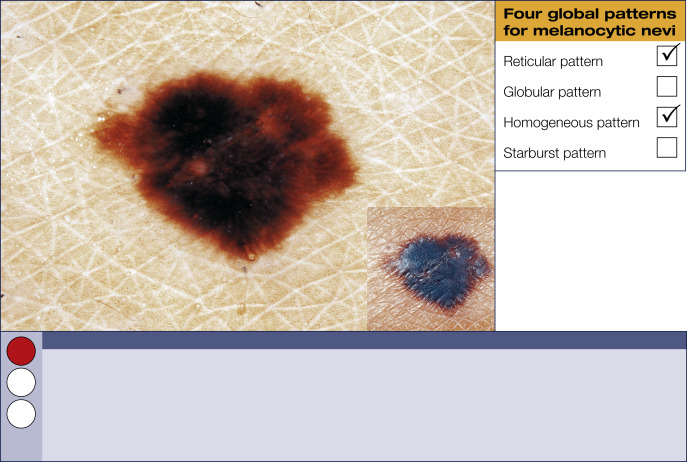
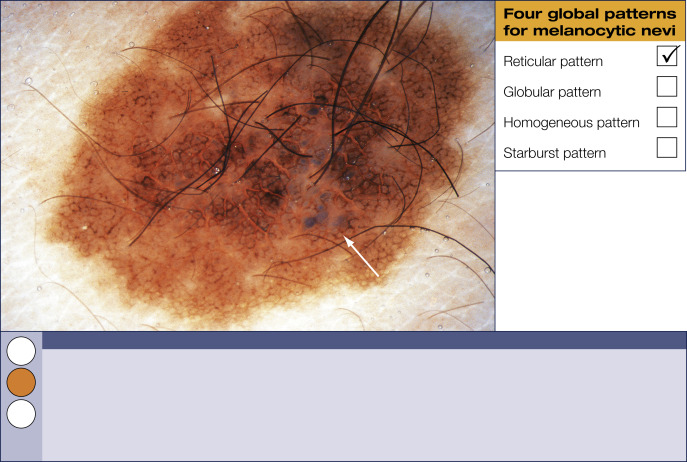
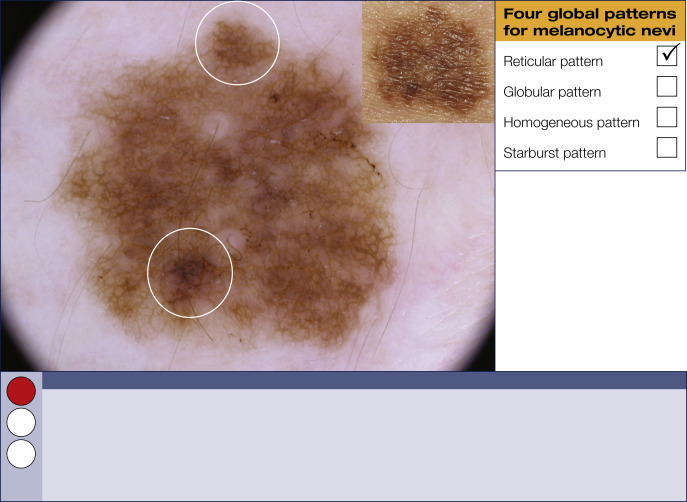
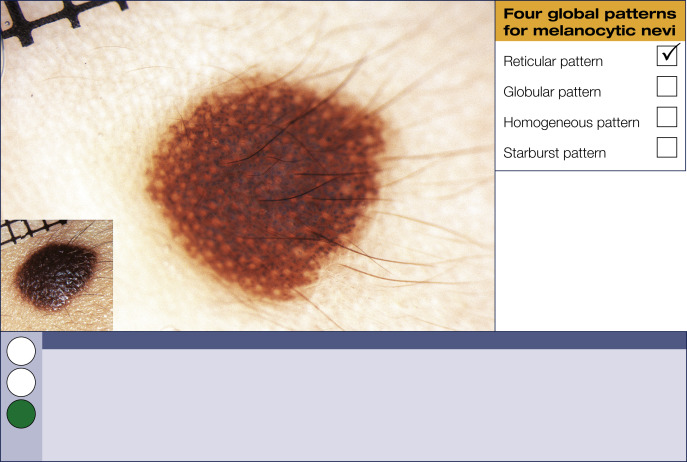
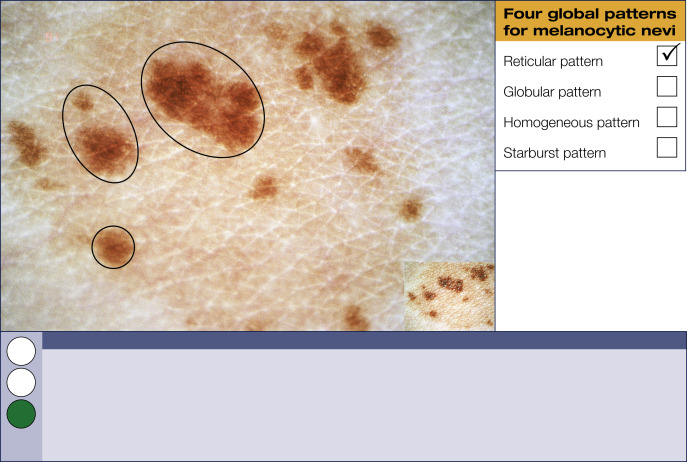
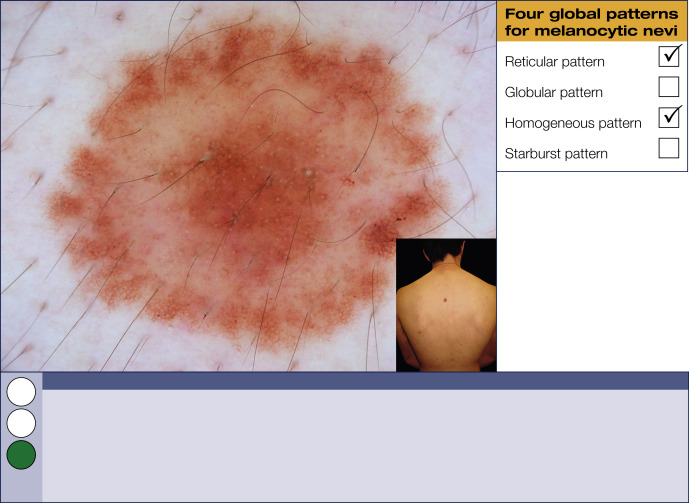
Reticular pattern
The reticular pattern is the most common global pattern in melanocytic lesions. It is characterized by a pigment network covering most parts of a lesion. The pigment network appears as a grid of line segments (honeycomb-like) in different shades of black, brown, or gray. Modifications of the pigment network vary with changes in the biologic behavior of melanocytic skin lesions, and these variations therefore merit special attention.
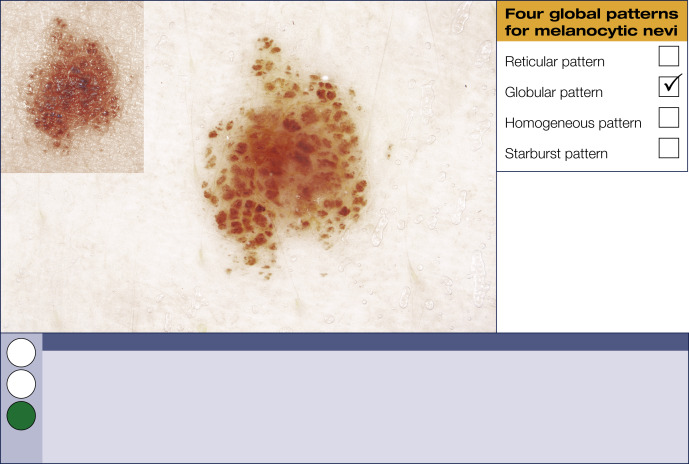
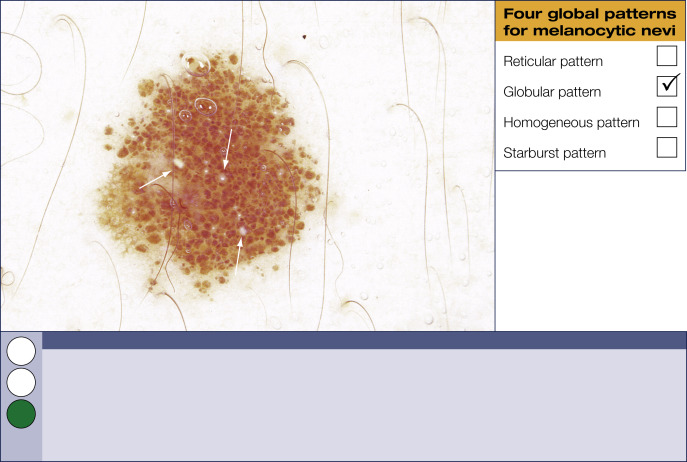
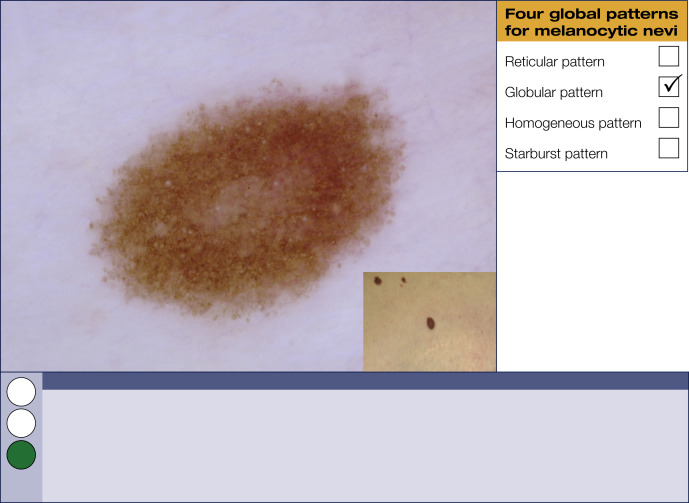
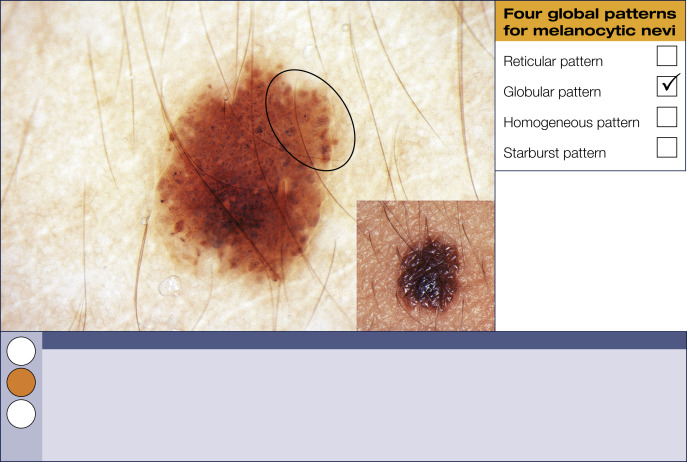
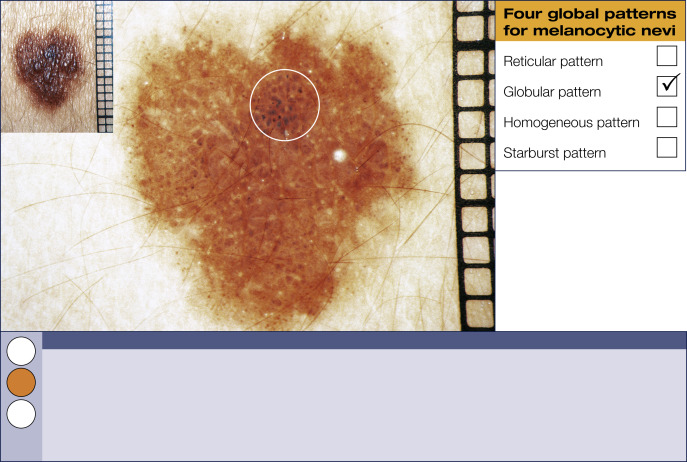
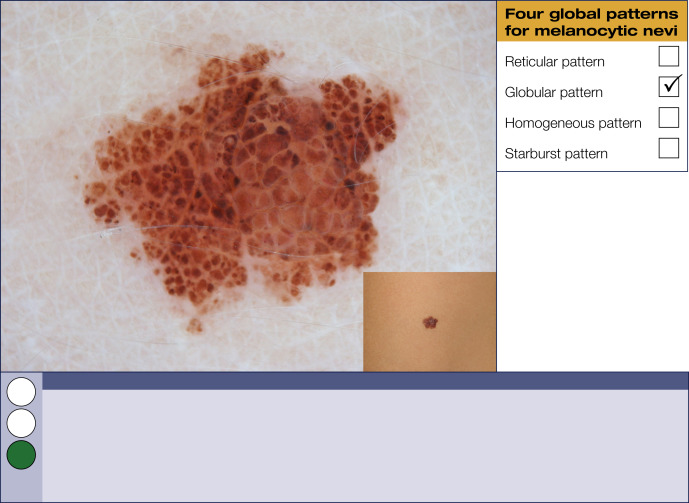
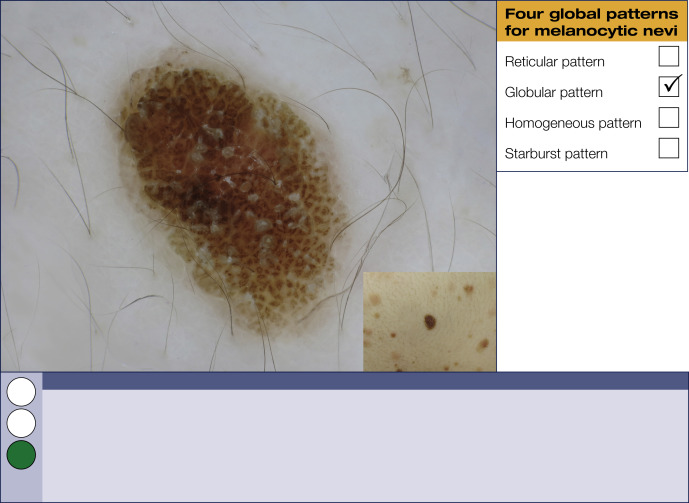
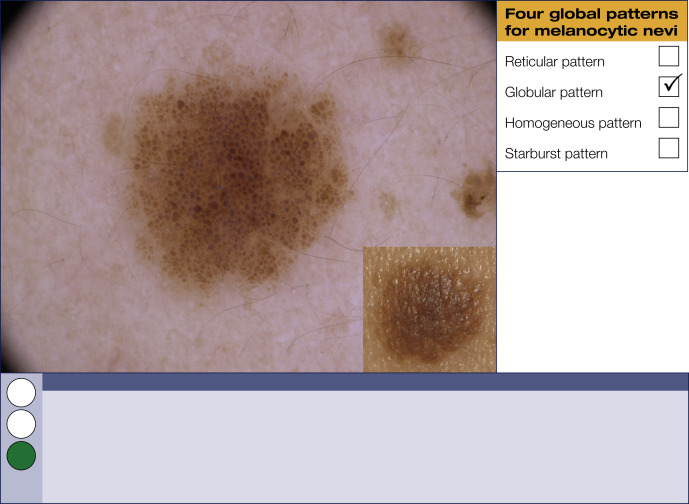
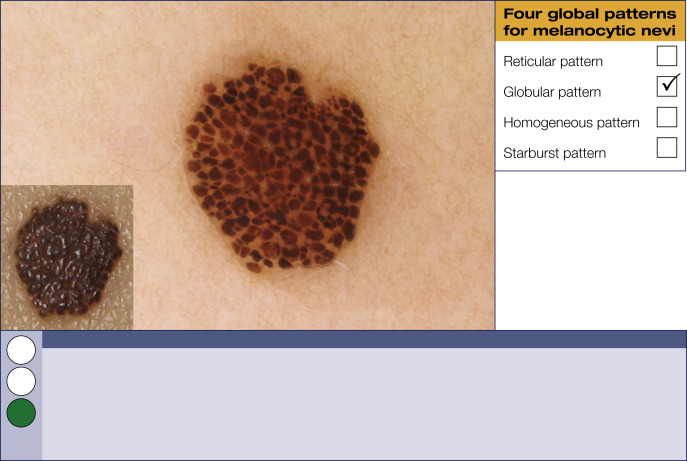
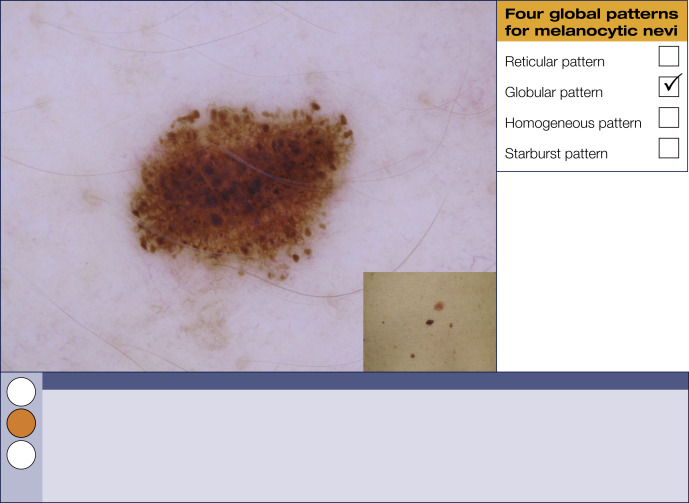
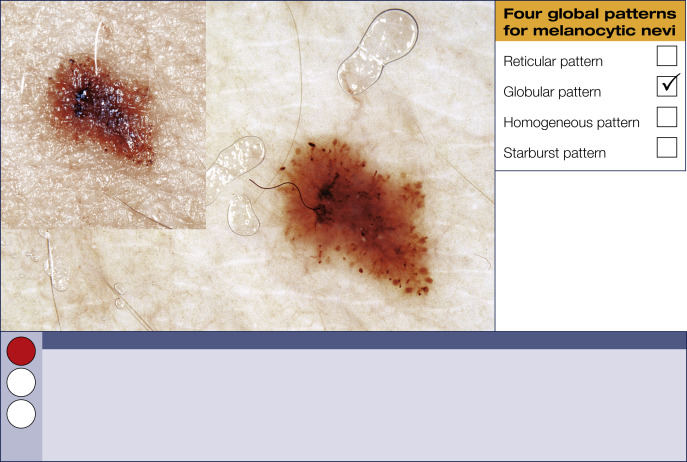
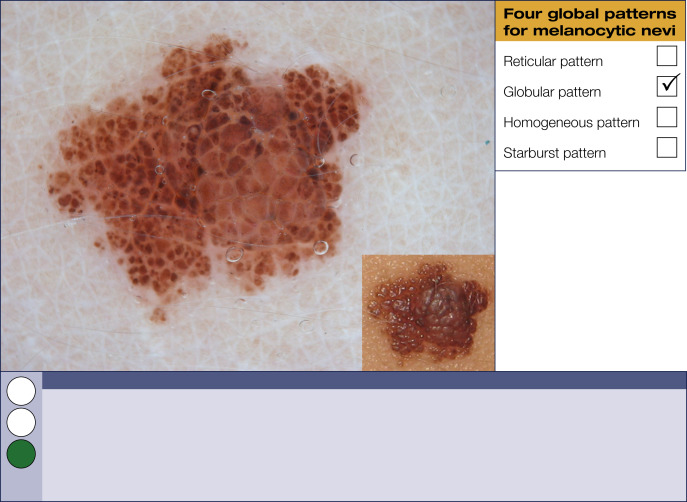
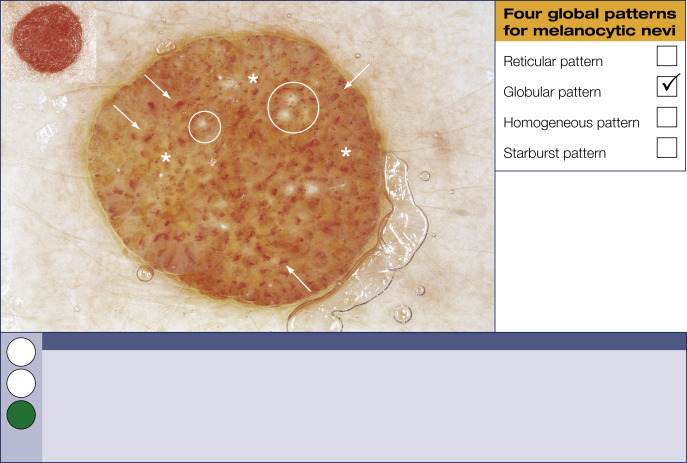
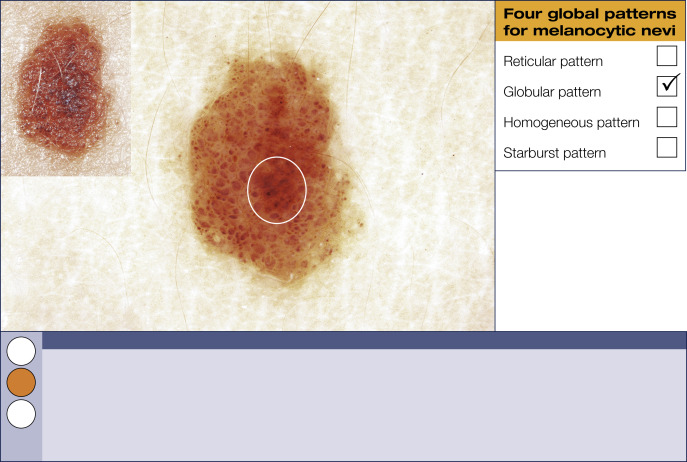
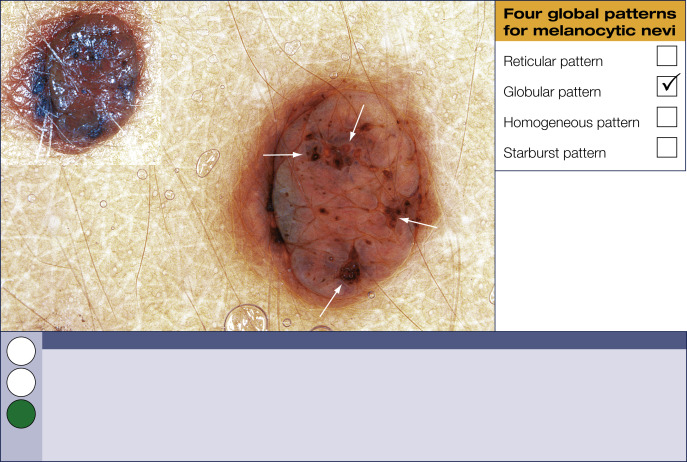
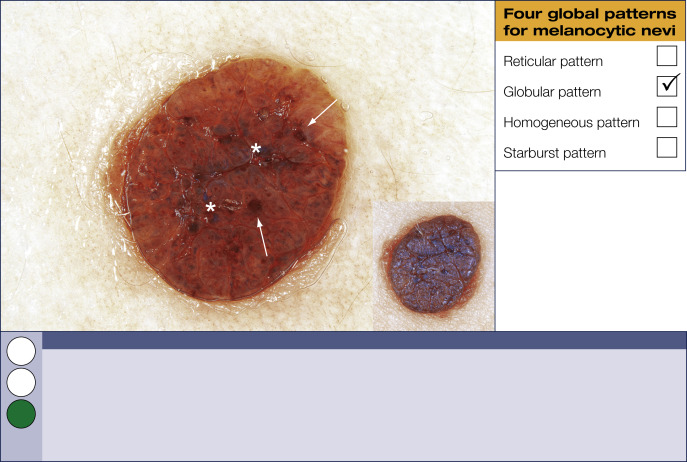
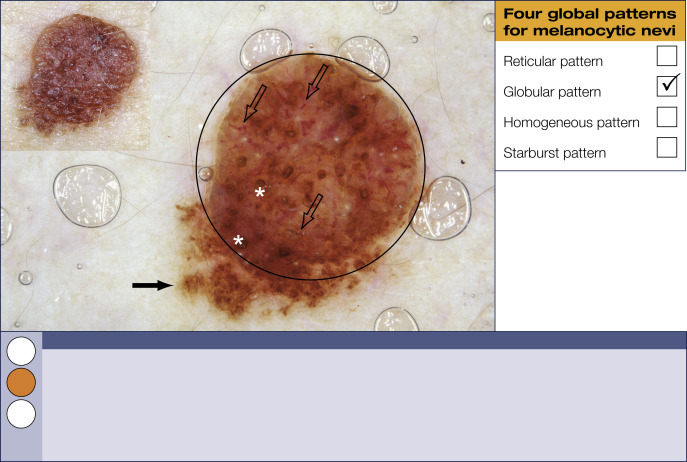
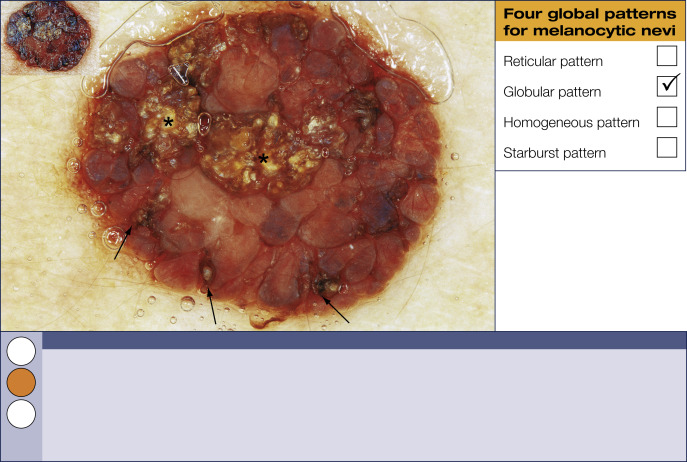
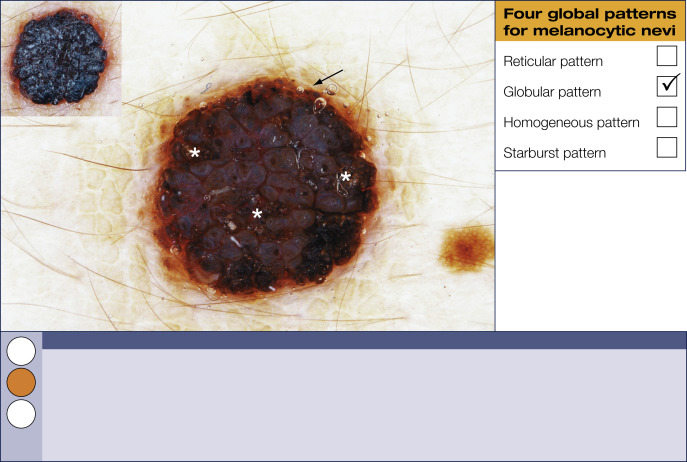
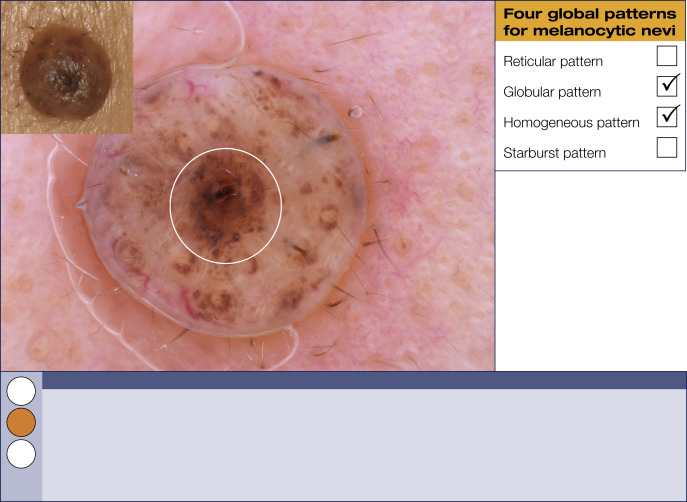
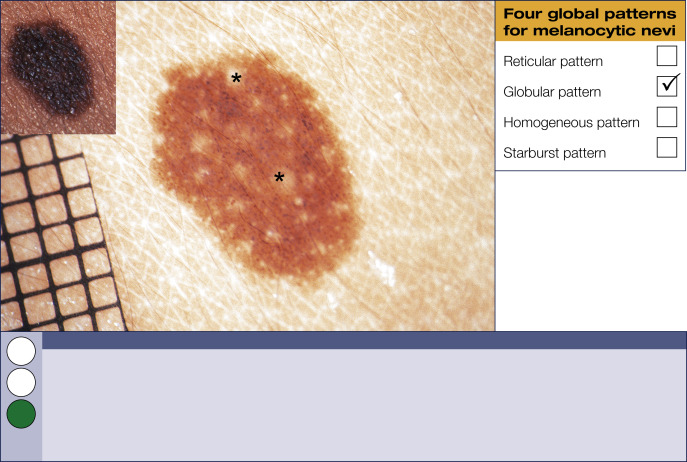
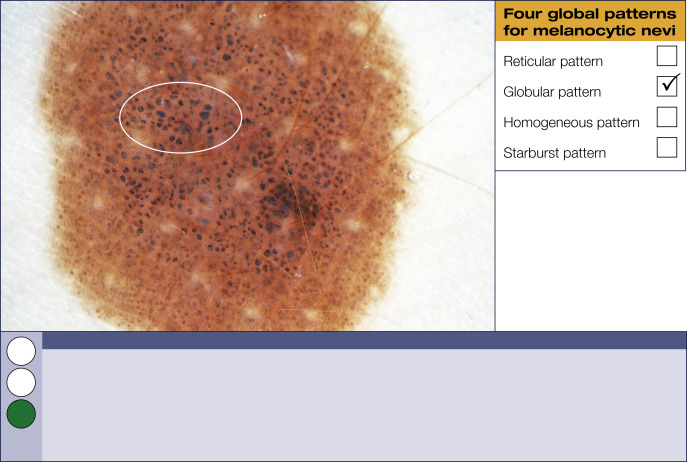
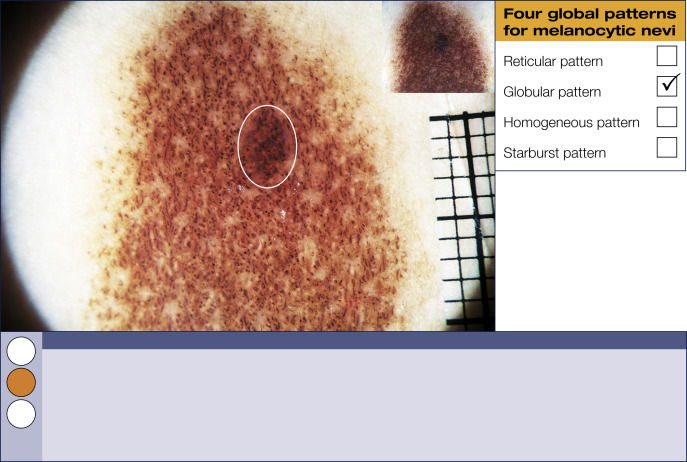
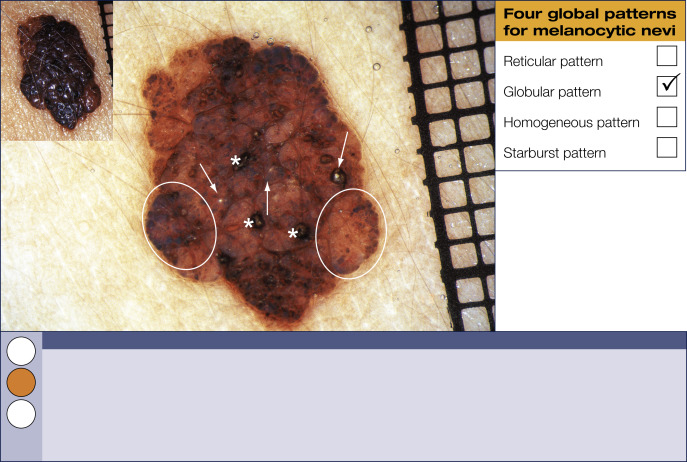
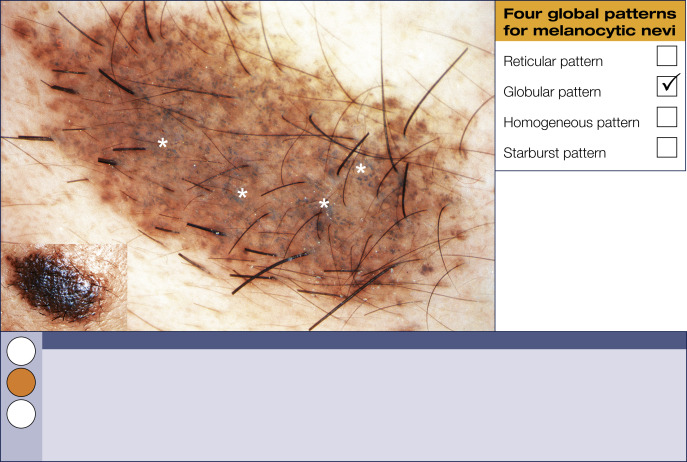
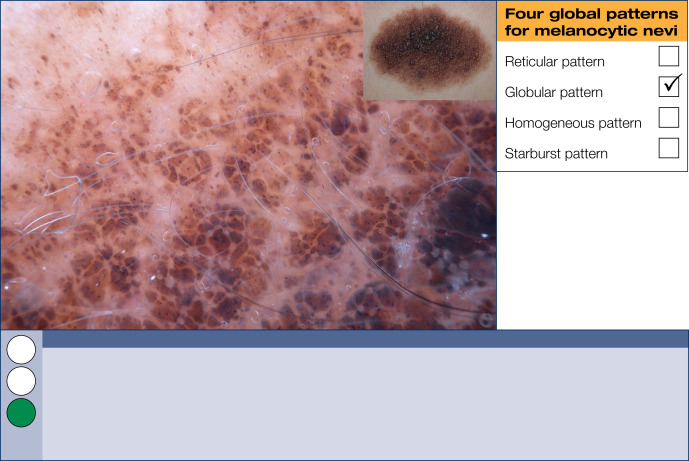
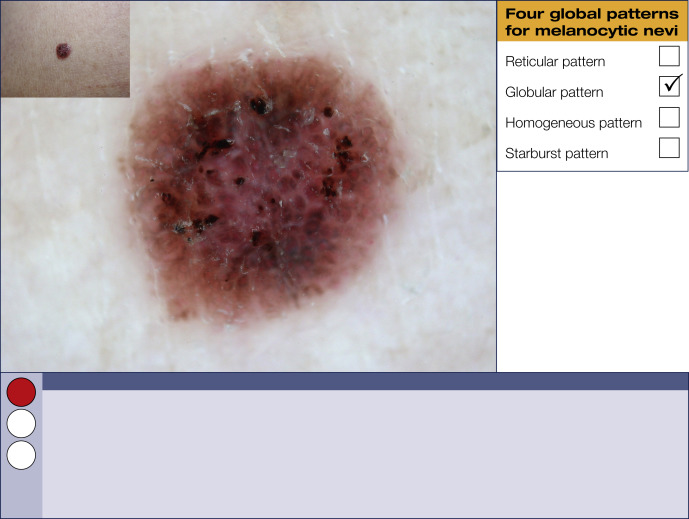
Globular pattern
Variously sized, round to oval brown structures fill these melanocytic lesions. This pattern can be found in congenital and acquired melanocytic and Clark (dysplastic) nevi.
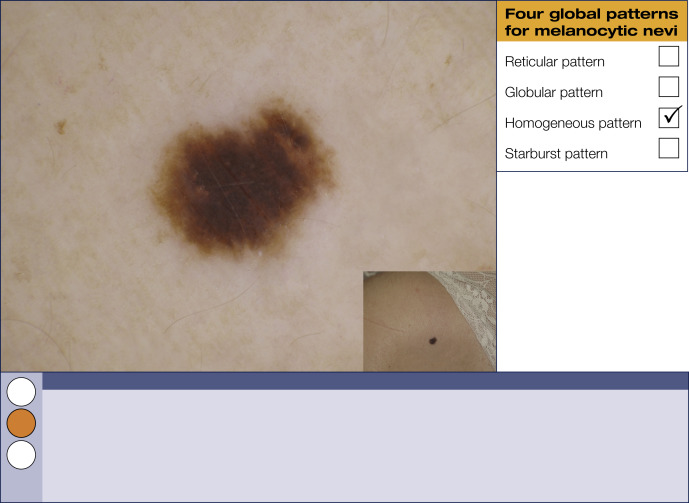
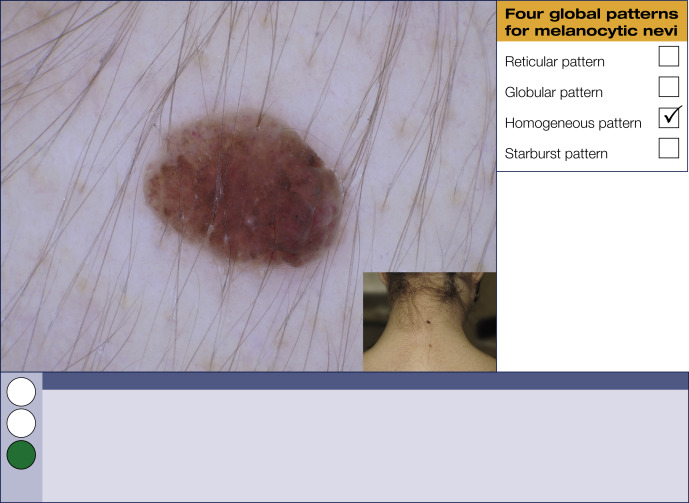
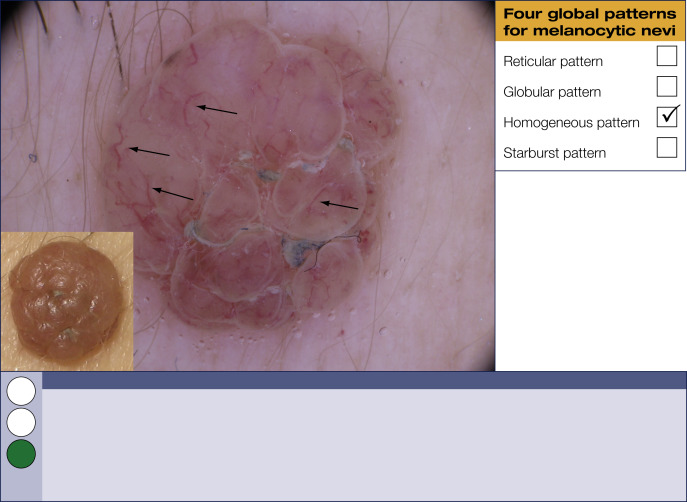
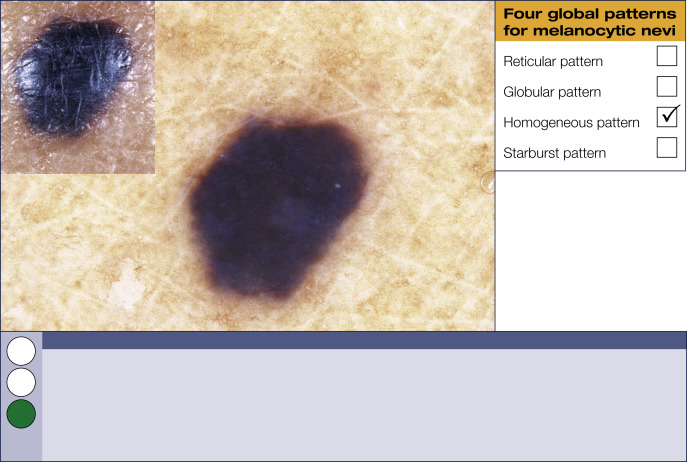
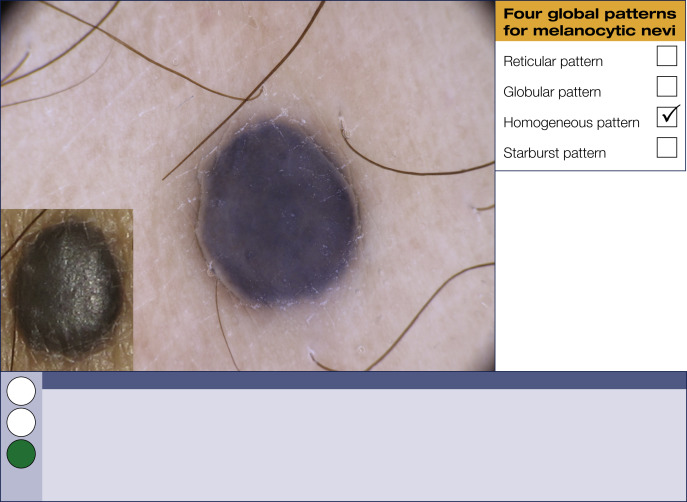
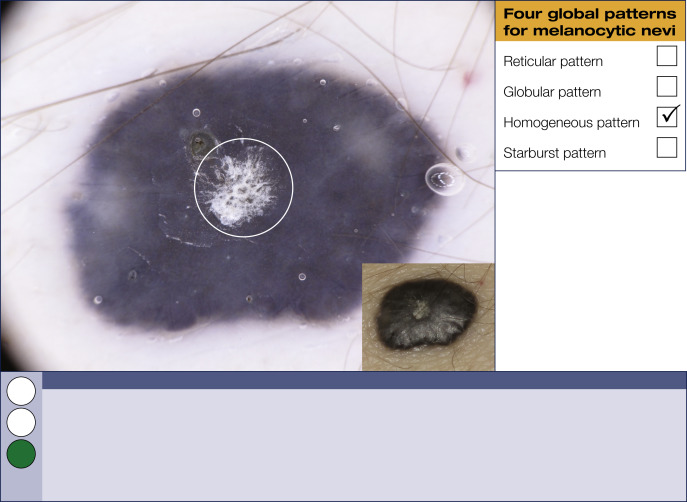
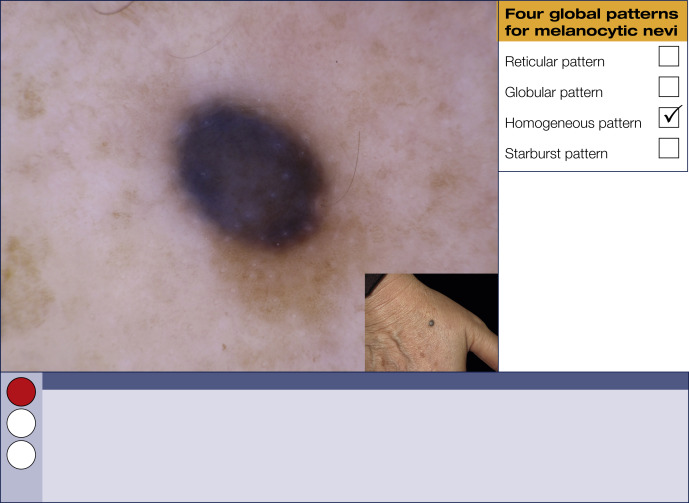
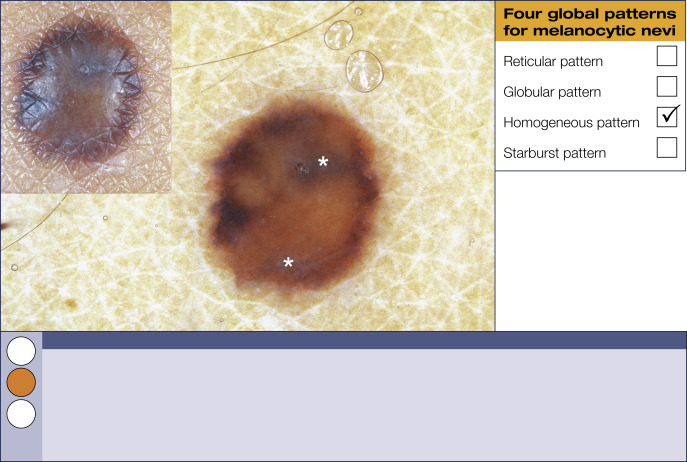
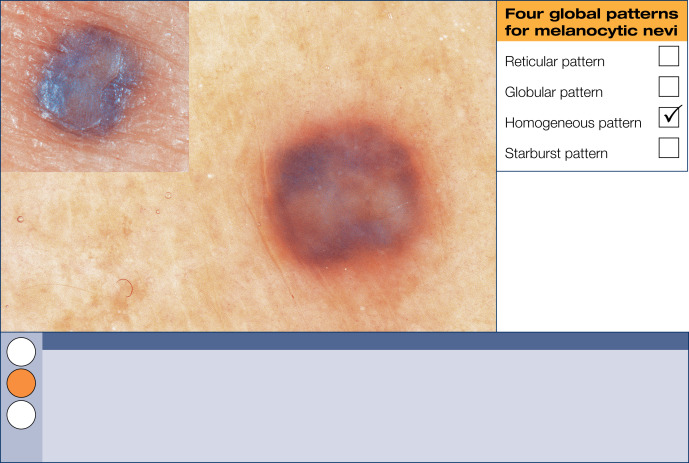
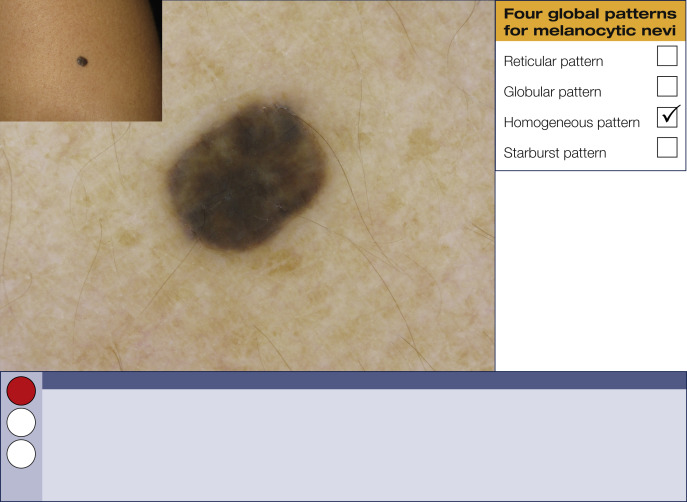
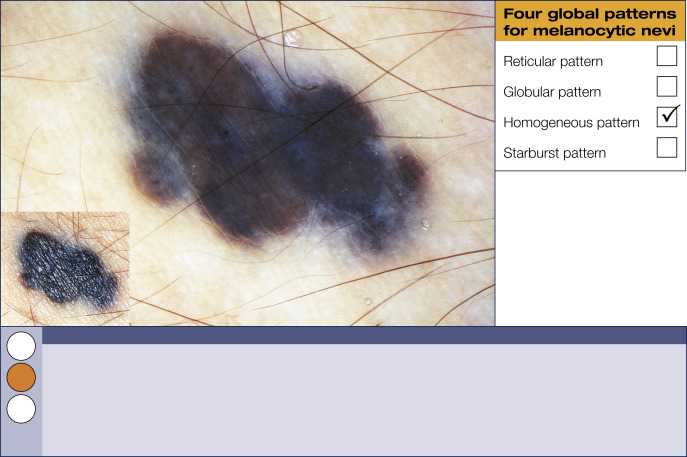
Homogeneous pattern
This pattern is characterized by a diffuse, uniform, structureless color filling most of the lesion. Colors include black, brown, gray, blue, white, or red. A predominantly bluish color is the morphologic hallmark of blue nevi.
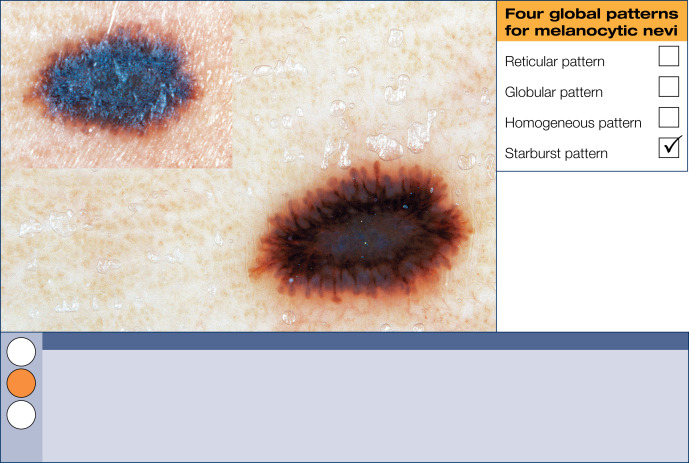
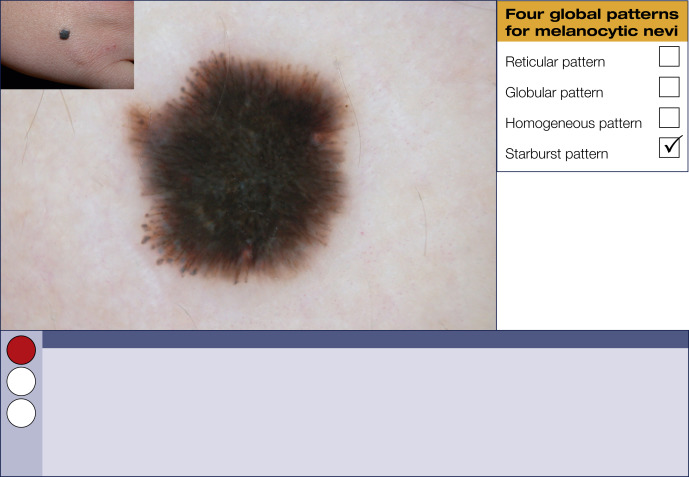
Starburst pattern
The starburst pattern is characterized by the presence of pigmented streaks and/or dots and globules in a radial arrangement at the periphery of a melanocytic lesion. This pattern is the stereotypical morphology in Spitz nevi.








Related posts:
 Introduction: The 3-point checklist: The short, easy way to avoid missing a melanoma using dermoscopy
Introduction: The 3-point checklist: The short, easy way to avoid missing a melanoma using dermoscopy
 Common clinical scenarios: Side-by-side comparisons of similar-appearing lesions that are benign or malignant
Common clinical scenarios: Side-by-side comparisons of similar-appearing lesions that are benign or malignant
 Therapeutic photomedicine
Therapeutic photomedicine
 White Lesions
White Lesions
 Neurocutaneous Disease
Neurocutaneous Disease
 15: Hand Cleansers and Sanitizers
15: Hand Cleansers and Sanitizers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


