(1)
Private Practice Fulya Teras, Istanbul, Turkey
1 Case Analysis: A Common Patient
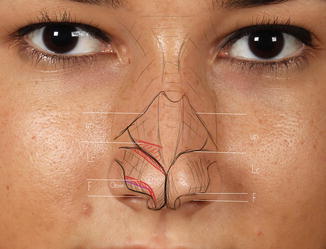
The patient does not have a facet polygon. The lateral crus is wide. The nose should be shortened, but the ala is floppy. The infralobule is too short and the upper lateral cartilage too long.




Lateral crus cephalic excision was not planned for the patient. The lateral crus will only be narrowed caudally. Rotation will be achieved with upper lateral cartilage caudal resection.
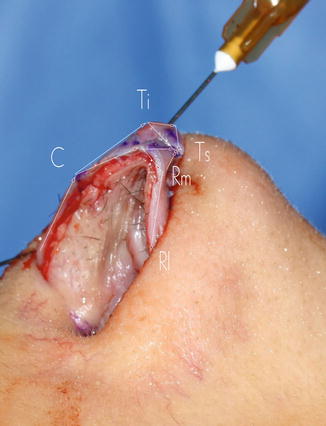
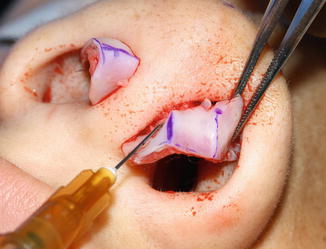
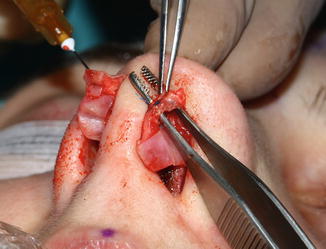
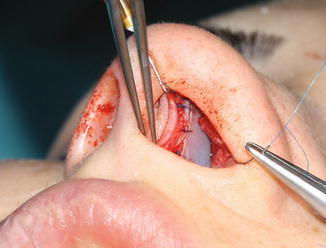
A three-stage incision has been performed safely. A 3 mm autorim flap has been made. An additional 2 mm resection will be made from the lateral crus.


A subperichondrial dissection has been performed.
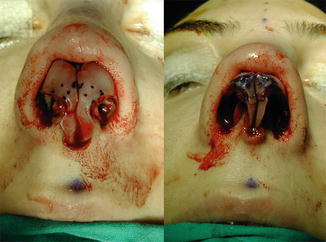
Nose tip cartilages were dissected. Another cartilage fold was seen on the lateral crus. The domes have been developed on the medial crura.


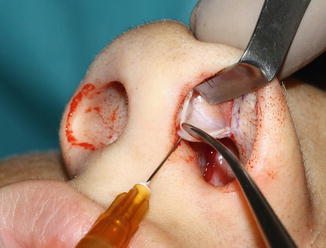
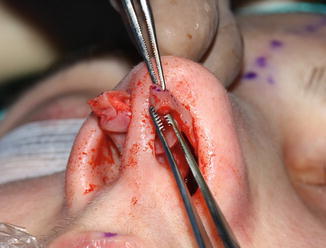
A 2 mm resection from the lateral crus caudal edge was planned.

A resection was made with scissors after cutting with the blade.

A resection (1–2 mm) was performed from the lateral crus caudal edge until rotation was achieved.
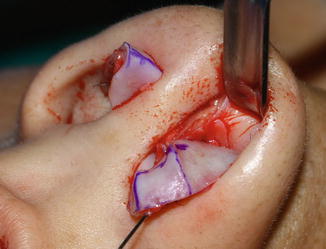

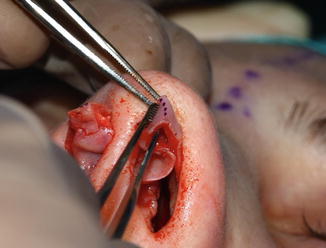
The second fold on the lateral crus was planned to constitute the dome. Tip surgery has been finished.

Alar edge resection has been performed for the floppy alae. The nostril was reduced using an avulsion flap.



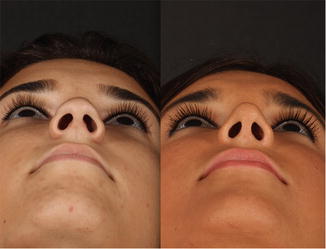
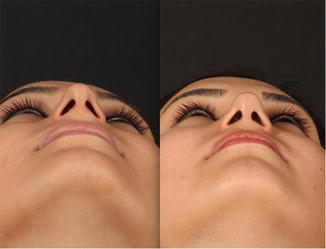
One-year photos of the patient.





2 Case Analysis: Thick Skin
In thick-skinned patients, the closed technique is more advantageous because of less nose tip edema. With the open technique, patients would be unhappy in the first months. While the patients were expecting a smaller nose, their nose would seem bigger due to edema. In these types of patients, in spite of diminishing soft tissue, we are trying to increase the highlights that are formed on the skin by repairing the Pitanguy and scroll ligaments.




Axis deviation to the left
Septum deviation to the right
Hump
Thick skin
Bulbous tip
Closed technique was applied. The septum’s caudal was dissected with a transfixion incision. The nasal dorsum was dissected in the subperichondrial and subperiosteal plane. The hump was resected. Excision was made from the septum base.
The domes were delivered through infracartilaginous incisions. A 3 mm cephalic incision was made, followed by a 1 mm caudal excision. A strut graft was then placed. A 4 mm steal was performed from the lateral crus. The lateral crus resting angle was fixed using the cephalic dome suture. The dog ears which formed at the caudal of the domes were resected.
A 3 mm medial crus overlap was performed. Low-to-low + external transverse osteotomies were performed. Libra grafts were utilized. Projection control suture.
Surplus mucosa was excised at the membranous septum and internal valve region. The septum was placed in the midline with scoring. In the end the depressor was excised.
3 Case Analysis: Thick and Oily Skin
The nose skin of patients who have a lot of oily pores will hardly adapt to the new anatomy. It is difficult to make oily noses smaller, and sometimes one surgery may not be enough. In thick-skinned noses, when the nose is reduced, the skin compresses like a bow and tries to return the nose to its previous shape during the healing period. In the first surgery that we performed on the patient below, the nose could not be reduced adequately. Axis deviation was corrected, but tip projection was not decreased enough. Surgery in this kind of patients can cause a long inflammatory period on the skin. Note the color change on the patient’s skin.



The second operation was performed one year later. These are the photographs one year after the second surgery. A fat injection was made to the patient’s forehead in order to make the nose appear smaller.
The columella can react better to nose reduction, but the alae cannot elevate the same amount. Projection was decreased. A resection was made from the alar bases. Alar edge resection was planned. In order to decrease the skin pores, oral vitamin A treatment was suggested.



The patient did not use vitamin A. In the third surgery, the nostril edge resection was performed. The nasal base was narrowed with external lateral osteotomy without dissection of the nose skin.
These are the patient’s photographs on the fourteenth day.



4 Case Analysis: Revision of My Own Case


The patient wanted a smaller nose. The tip was narrow and there existed a depression on the infralobule. A cartilage hump is still seen. I made the first surgery using the open technique. Below there is a view of the cartilages at the beginning and after surgery. I did not shorten the lateral crus enough to decrease the rotation and projection. The resting angle was not corrected adequately. Before changing to the cephalic dome suture technique in 2008, my technique was creating dome triangles with two separate dome sutures. But this technique is not sufficient for correcting the resting angle. I used this doubled dome suture only for a short time, since its planning and execution are difficult.
The closed technique was used. The septum’s caudal was dissected with a transfixion incision. A wide dissection was made until the maxilla. The nasal dorsum was dissected in the subperichondrial and subperiosteal plane. The cartilage hump was resected extramucosally.
A 2 mm autorim flap and a 1 mm lateral crus caudal excision were performed. A 3 mm cephalic excision was made from the lateral crura. Both on the right and left did I perform a 4 mm lateral crus steal. Then a 5 mm medial crus overlap was performed. The lateral crus resting angle was corrected by the cephalic dome suture.
Three strut grafts were inserted. The Ti point was supported by the medial crural strut grafts. The infracartilaginous incision was repaired.
The bone osteotomy line was reduced by means of a Çakir 90 chisel, and Sheen spreader grafts were used.
By means of cartilage and mucosa resections from the caudal septum, the nose was shortened. The dermocartilaginous ligament was repaired in the first surgery. The integrity of the repaired dermocartilaginous ligament did not deteriorate.

After four years we could perform a subperichondrial dissection on our patient. The revision of the subperichondrial dissection was much easier.

You can see the Pitanguy ligament below repaired with a 6/0 Prolene suture.
The new placement of the domes was determined. A 4 mm steal was performed, causing increase in rotation and decrease in tip projection while the nose was shortened.
A 5 mm medial crus overlap was made. As a result the infralobule was shortened by 1 mm. The footplates were set back posteriorly with the transfixion incision, and columella projection was decreased.



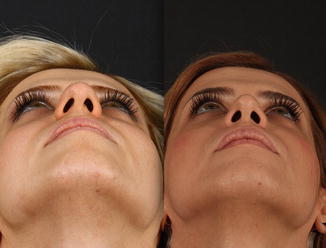
Photographs of the patient six months after revision.




The effect of footplate setback can be seen clearly in the basal view.

Because of the autorim flap, the caudal edge highlight of the lateral crus has become more obvious.

5 Case Analysis: Thick Skin and Large Hump
In this kind of patients, the skin is too loose for the new nose. Excess skin can accumulate in the supra-tip region. In addition, alar resection was applied to the patient. Alar resection is also important for the smaller appearance of the patient’s nose. The patient’s infralobule polygon is short; therefore, with the lateral steal procedure, used for rotation, the infralobule will extend. Left axis and tip deviation exists. Below are the first-year photographs.






Septum deviation to the left, axis deviation to the left.
Wide nasal base, wide nose alae.
Thick skin.
Bulbous tip.
Closed technique.
Hump was resected.
The excision was made from the septum base.
The domes were delivered through an infracartilaginous incision.
A 2 mm cephalic excision was made from the lateral crus.
Left lateral crus steal of 2 mm.
Right lateral crus steal of 3 mm.
A 2 mm lateral crus caudal excision was performed.
A strut graft was inserted.
The lateral crus resting angle was fixed using the cephalic dome suture.
Internal high-to-low osteotomy + external transvers osteotomy.
Spreader flaps.
Projection control suture.
The footplates were sutured to each other with 5/0 Prolene.
Left levator was dissected.
Rim grafts were placed.
The nostrils and alae were reduced using the avulsion flap and elliptic resection.
6 Case Analysis: Closed Approach Healing Rate
The patient has a 2–3 mm hump. Her skin is thin and her tip low. The patient needs a good rotation. It is necessary to do more steal from the lateral crus. The left dome is lower, and tip asymmetry is observable. Hence it will be necessary to steal more from the left than the right one. The patient’s infralobule polygon is not very short. As stealing from the lateral crus increases the infralobule, a medial crus overlap will be needed. As the patient’s depressor is active, strut grafts can be used more than once. Moreover, caudal resection of the upper lateral cartilage was planned for nose shortening and rotation. We determine the amount of resection at the end of surgery. Before closing the intercartilaginous incision, we resect the previously protruding upper lateral cartilage. The patient’s footplate polygon is wide. It might not be enough to resect the septum inside. Soft tissue resection between the footplates will be required. Below you can see the patient’s one-year photographs.





Closed technique was used.
One millimeter of the caudal septum was left on the columellar side.
Wide dissection was made until the maxilla.
Hump was resected extramucosally.
A 1 mm autorim flap and a 2 mm lateral crus caudal excision were performed.
A 3 mm cephalic excision was made from the lateral crus.

Left lateral crus steal of 6 mm.
Right lateral crus steal of 5 mm.
Medial crus 3 mm overlap.

The lateral crus resting angle was fixed with a cephalic dome suture.


By making two cuts on the lateral crus, the scroll facets were created. You can see the Pitanguy midline ligament in between. A posterior strut graft was sutured to the septum.

Three strut grafts were placed.
Upper lateral cartilage caudal excision 4 mm.
The bone osteotomy line was reduced with a Çakır 90 chisel and bone rasp.
Libra grafts were placed.
The footplates were sutured to each other with 5/0 PDS.
7 Case Analysis: Supratip Healing Period
Leaving the Pitanguy ligament intact and repairing the scroll ligament can create an obvious depression in the supratip region. The effect of an intact Pitanguy midline ligament can become noticeable if edema in the lip region pushes the nose tip further than its position in surgery. This is generally a temporary effect and requires some waiting. Protecting the Pitanguy ligament in thin-skinned patients can cause a depression that will require revision. During surgery, if the supratip breakpoint is obvious, I dissect between the superficial SMAS and the Pitanguy wider than normal. If this is not enough, then I use cartilage chips grafts.

The patient’s six-month photographs.






Appearance of the cartilages before tip surgery.

Appearance of the cartilages after tip surgery.

Hump.
Low tip.
Thin skin.
Closed technique.
One millimeter of the caudal septum was left on the columellar side.
Nasal dorsum was dissected in the subperichondrial and subperiosteal plane.
Three millimeter lateral crus cephalic excision.
Two millimeter lateral crus caudal excision
Left lateral crus steal of 3 mm.
Right lateral crus steal of 3 mm.
Medial crus 2 mm caudal excision.
Partial medial crus overlap.
Three strut grafts were put.
Diced grafts for the tip.
The lateral crus resting angle was corrected using a cephalic dome suture.
Lateral osteoectomy.
Libra grafts were placed.
Columellar cartilage was sutured to the septum.
Dermocartilaginous ligament was kept intact.
Scroll ligament was sutured to the septum perichondrium.
Cartilage chips were placed on the nasal dorsum, and the nose radix was elevated.
The footplates were sutured to each other with 5/0 PDS.
8 Case Analysis: Wide Dorsum, Wide Radix, Bulbous Overprojected Tip
Below are the patient’s second-year photographs after surgery. A revision was planned for our patient. I have decreased the patient’s tip projection by moving the footplates posteriorly, but I did not shorten the lateral crus enough. As the infralobule polygon length is adequate, I am planning to make a 3 mm lateral crural steal and 3 mm medial crus overlap. Thus, without changing the infralobule length, rotation will be possible.






8.1 First Surgery
Closed technique.
Nasal dorsum was dissected in the subperichondrial and subperiosteal planes.
Hump was resected.
Excision was made on septum base.
The domes were delivered through an infracartilaginous incision.
Cephalic excision was made from the lateral crus.
A 3 mm lateral crural caudal excision was performed.
A strut graft was inserted.
A 2 mm dome cephalic excision was made.
The lateral crus resting angle was corrected using the cephalic dome suture.
Osteotomy low-to-low + external transverse.
Libra grafts were inserted.
Projection control suture.
Dermocartilaginous ligament was repaired.
Cartilage chips were placed on nasal dorsum.
Mucosa of the scroll region was sutured with dermocartilaginous ligament and supported.
Excess mucosa in membranous septum and internal valve region were excised.
Z-plasty was applied to the nostril base.
8.2 Second-Year Revision
Closed technique
Middle of the septum caudal was put forward with transfixation incision.
One millimeter of caudal septum was left in the columella.
A wide dissection was made until the maxilla.
Nasal dorsum was dissected at subperichondrial and subperiosteal plane.
A graft was taken from the septum.
Note
As I had not performed an L septoplasty in the first surgery, there was enough graft in the septum.
Domes were delivered with rim incision.
Autorim flap: 2 mm.
Lateral crus caudal excision: 1 mm.
Note
It is possible to perform an autorim flap in patients who have a revision.
Another lateral steal was planned, but not performed due to fibrosis. A 3 mm overlap was applied to the lateral crus near the dome.
A 4 mm incision was made for the scroll section.
The domes’ positions were fixed by means of a cephalic dome suture.
One strut graft was inserted.
Bone osteotomy lines were reduced with a Çakır 90 chisel. Bone rasp. Osteotomy was applied in the first surgery.
Sheen spreader graft to the right.
Columellar cartilage was sutured to the septum.
The dermocartilaginous ligament is intact.
The scroll ligament was sutured to the septum perichondrium.
Cartilage chips and rasped bone were placed for dorsal camouflage.
Internal valve region mucosa was sutured with the scroll ligament and supported.
Nostrils were reduced.
Let’s examine the second surgery photographs.
In the previous surgery an infracartilaginous incision had been made. Now a 2 mm autorim flap was performed.









