The most challenging and instrumental step in achieving harmonious form and function during rhinoplasty is the successful completion of osteotomies. Osteotomies are performed to correct deformities of the bony nasal vault. Successful treatment of deformity of the bony vault is achieved through organized thinking, comprehensive knowledge of nasal anatomy, and thorough preoperative and intraoperative planning. In this review the authors discuss the pertinent anatomy, technical considerations, and complications that rhinoplasty surgeons should be aware of to optimize the correction of deformities of the nasal bony vault.
Rhinoplasty remains to be one of the most challenging facial plastic surgical procedures performed. The surgeon seeks to achieve the combination of aesthetic harmony with the surrounding facial features and preservation or development of nasal function and support. One of the most challenging and instrumental steps in achieving harmonious form and function during rhinoplasty is the successful completion of osteotomies. Osteotomies are performed to correct deformities of the bony nasal vault. Successful treatment of deformities of the bony vault is achieved through organized thinking, comprehensive knowledge of nasal anatomy, and thorough careful preoperative and intraoperative planning. In this review the authors discuss the pertinent anatomy, technical considerations, including selection of various osteotomy techniques, and complications that rhinoplasty surgeons should be aware of to optimize correction of deformities of the nasal bony vault.
Anatomy
The bony framework of the external nose consists of the paired nasal bones and the ascending processes of the maxilla. The nasal bones are thick cephalically where they articulate with the frontal bone, and are thin as they extend inferolaterally where they articulate with the maxilla and the upper lateral cartilage. This variability in thickness is important for consideration of placement of the osteotomies. For example, the lateral osteotomy should be placed in the thicker ascending process of the maxilla instead of the thin lateral nasal bone.
The nasal bones are supported by their articulation superiorly with the frontal bone at the nasofrontal suture line (nasion), laterally at the ascending process of the maxilla and in the posterior-midline where the bones are fused with the perpendicular plate of the ethmoid. It is important to consider the midline attachment to the perpendicular plate while treating the twisted nose deformity. In patients with this deformity, the nasal bones and ethmoid plate are deviated and the nasal bones may have variable symmetry, with one side being longer than the other. The surgeon must address the nasal bones and the deviated bony septum. If the deviation at the perpendicular plate is not treated, the patient will often have persisting deviation of the bony vault.
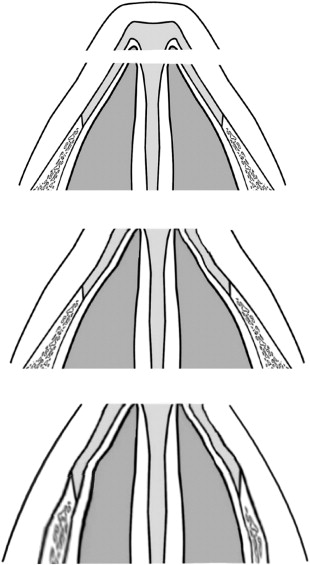
Inferiorly the nasal bones overlap the cephalic margins of the upper lateral cartilages, providing support to the cartilaginous middle vault. Thus, narrowing of the nose by infracture of the bony sidewall will also result in the narrowing of the middle third caused by this connection between the nasal bones and upper lateral cartilage. The surgeon should be aware of this especially after hump reduction, where the width of the broad native dorsal septum is significantly narrowed ( Fig. 1 ). The resultant upper and middle vault narrowing may lead to profound obstruction in patients who already have a narrow bony base or when the base is significantly narrowed through lateral osteotomies with medial displacement of the bony base.
One must also take care to preserve the articulation of the nasal bones and upper lateral cartilage during dissection or rasping near the inferior edge of the nasal bones. Disruption of this junction will result in collapse of the upper lateral cartilage and a resulting depression of the middle vault that is difficult to correct. Rasping at the inferior medial edge of the nasal bone makes the superior medial edge of the upper lateral cartilage prominent; this is due to the flexible character of the cartilage, which may disarticulate and bend outward. This anomaly should be corrected as it may cause a persistent fullness after surgery.
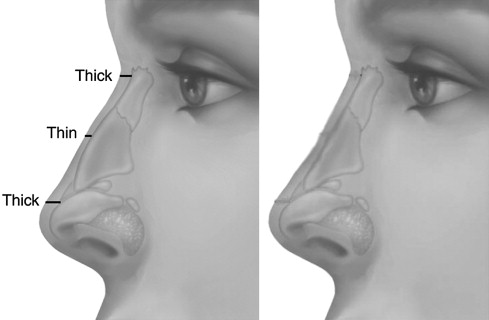
The soft tissues overlying the bony framework include the skin, subcutaneous tissues, superficial musculoaponeurotic system, and periosteum. The relationship between the soft tissues and the underlying bony framework determines the overall contour of the nose, thus a comprehensive knowledge of these structures is required to achieve optimal results when altering the bony framework of the nose. The soft-tissue envelope varies in thickness over the dorsum of the nose ( Fig. 2 ). The skin and subcutaneous tissues are thicker superiorly in the area of the nasion and inferiorly at the supratip. The soft tissue thins over the rhinion, the osseocartilaginous junction of the nasal bones, and the upper lateral cartilages. Thus, when altering the bony profile, a slight hump should remain at this junction to give an overall straight appearance of the profile. If the bony profile is straight there will be a small “saddle-nose” appearance when the soft tissues are redraped (see Fig. 2 ).
The periosteum represents the layer between the soft-tissue envelope and the underlying bony framework. It is important to use caution while raising the adherent periosteum from the nasal bones, because preserving the periosteum as an intact layer will provide a thicker flap, which provides better camouflage over the newly reconstructed bony framework. Raising the periosteum with the flap also decreases the risk for postoperative trophic changes. Minimal lateral elevation of the periosteum should be performed to preserve the periosteal attachments to the ascending process of the maxilla. This action will help stabilize the bony fragments after performing lateral osteotomies.
It is important to have a thorough understanding of the relationship between the bony/cartilaginous, and soft-tissue architecture of the nose. It is also important to understand the changes that occur in the bony framework with age. While performing osteotomies on young patients the nasal bones are soft and may result in greenstick fractures. These fractures are incomplete, making mobilization of the fragment difficult, therefore in younger patients continuous osteotomies are generally preferred to help avoid greenstick fractures and ensure proper mobilization. Older patients tend to have brittle bones or may have a history of previous fractures or surgeries that can lead to comminution while osteotomies are performed. In older patients one may preferably create greenstick fractures or incomplete osteotomies, with digital completion of the osteotomy in order to avoid comminution of the bony fragment.
It is also important to consider a patient’s age when determining the degree of anatomic change that is to be created. Older patients have grown accustomed to their appearance and will be more affected by significant alterations in their appearance. It is best to perform more conservative alterations to the bony framework in older patients. Younger patients tend to be more accepting of significant changes to their nasal appearance.
Evaluation of bony vault
With all aspects of rhinoplasty, proper preoperative analysis is critical to obtaining optimal results. It is imperative to correctly determine the patient’s deformities so that the most effective techniques for correction of these deformities may be performed. One should be able to visualize and palpate the external anatomy, and at the same time predict the underlying structure that determines the external appearance. Complete nasal and facial analysis is essential as the appearance of the bony vault must be in balance with the other aspects of the nose and the rest of the face. During nasal analysis, the nose is divided into vertical thirds with the upper one-third representing the bony nasal vault.
On anterior evaluation the overall alignment, length, and width of the bony vault should be determined. Alignment of the bony dorsum may be evaluated by determining a relative midline of the nose. A line defined by the mentum, upper incisors, philtrum, and glabella may be used to determine the midline. Deviation toward the right or the left should be determined in relation to this line and any continued deviation into the middle or lower one-thirds. Ideally the dorsum of the nose would be straight and symmetric on either side of this midline. Asymmetries may be caused by deviations of the bony vault toward one side of the nose or may be due to the width irregularities between the upper and middle one-thirds of the nose.
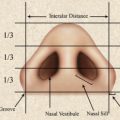
The width of the bony vault should be analyzed to include the width at the nasal facial sulcus or bony base and also at the dorsal ridge. The ideal width is influenced by features such as nasal length, projection, skin thickness, and other facial proportions, and will vary depending on the individual. The width of the nasal dorsum should be approximately two-thirds of the width of the alar base, which should approximate the intercanthal distance ( Fig. 3 ).
The nasal bones and ascending process of the maxilla are palpated for irregularities. Previous fractures because of trauma or previous surgery with their associated inward or outward displacement may be palpated. The bones should be assessed for a concave or convex shape as this may require an intermediate osteotomy to correct the associated deformity. Significant differences in the height of the nasal bones should also be evaluated, as this will often occur in crooked nose deformities.
The profile evaluation of the bony dorsum determines the level of the radix, the nasofrontal angle, and dorsal alignment. The radix or root of the nose corresponds to the junction of the nasal and frontal bones, and this should be located at the level of the supratarsal crease. The nasofrontal angle, defined by glabella-to-nasion line intersecting with nasion-to-tip line, should be between 115° and 130°. A high radix or shallow nasofrontal angle may require rasping in order to improve the contour in this area. The desired change may be achieved through rasping; however, this change often becomes muted through healing, and long-term deepening of the radix is difficult to accomplish. Occasionally a transverse osteotomy at the nasal root may be performed to push down this area and deepen the radix. On the other hand, a low radix may accentuate the appearance of a dorsal hump, and this should be identified so that the surgeon may augment the radix with a graft, thus reducing the amount of hump to be removed. It is also important to determine the appropriate tip projection and rotation in evaluating the bony profile alignment. The tip and radix position will influence the dorsal height required to achieve an aesthetically pleasing profile.
It is important to include an intranasal evaluation for complete assessment of the bony vault. Collapsed nasal bones will be evident as they cause impingement of the airway and are often associated with the collapse of the attached upper lateral cartilage. This may contribute to decreased patency at the internal valve as the upper lateral cartilage collapses toward the septum. Patients who have had previous placed “low to low” osteotomies with medialization at pyriform aperture may present with nasal valve obstruction as well. The degree of airway impingement with this type of osteotomy will be accentuated in patients with preexisting narrow pyriform apertures, hypertrophied inferior turbinates, or long nasal bones.
Evaluation of bony vault
With all aspects of rhinoplasty, proper preoperative analysis is critical to obtaining optimal results. It is imperative to correctly determine the patient’s deformities so that the most effective techniques for correction of these deformities may be performed. One should be able to visualize and palpate the external anatomy, and at the same time predict the underlying structure that determines the external appearance. Complete nasal and facial analysis is essential as the appearance of the bony vault must be in balance with the other aspects of the nose and the rest of the face. During nasal analysis, the nose is divided into vertical thirds with the upper one-third representing the bony nasal vault.
On anterior evaluation the overall alignment, length, and width of the bony vault should be determined. Alignment of the bony dorsum may be evaluated by determining a relative midline of the nose. A line defined by the mentum, upper incisors, philtrum, and glabella may be used to determine the midline. Deviation toward the right or the left should be determined in relation to this line and any continued deviation into the middle or lower one-thirds. Ideally the dorsum of the nose would be straight and symmetric on either side of this midline. Asymmetries may be caused by deviations of the bony vault toward one side of the nose or may be due to the width irregularities between the upper and middle one-thirds of the nose.
The width of the bony vault should be analyzed to include the width at the nasal facial sulcus or bony base and also at the dorsal ridge. The ideal width is influenced by features such as nasal length, projection, skin thickness, and other facial proportions, and will vary depending on the individual. The width of the nasal dorsum should be approximately two-thirds of the width of the alar base, which should approximate the intercanthal distance ( Fig. 3 ).