Osteocutaneous Parascapular Flap for Mandibular Reconstruction
Ravi K. Garg
John W. Siebert
DEFINITION
The parascapular osteocutaneous free flap serves as a versatile reconstructive option for composite head and neck defects involving the mandible.
The lateral border and angle of the scapula are the most commonly used osseous flap components, although harvest of the medial scapular border has also been described.
Soft tissue elements that may be incorporated into the flap include skin, fat, fascia, muscle such as the serratus and latissimus, and nerves, including the thoracodorsal nerve.
ANATOMY
The parascapular osteocutaneous free flap is based on the subscapular system emerging from the distal third of the axillary artery.
The circumflex scapular artery branches from the subscapular artery and serves as the primary blood supply to the parascapular osteocutaneous flap.
The circumflex scapular artery can be reliably identified in the triangular fossa, which is bound by the teres major and minor muscles as well as the long head of the triceps (FIG 1).
The thoracodorsal artery also branches from the subscapular artery and sends a branch to the scapular angle either directly or as a side branch of the serratus muscle branch.
The angular artery can be useful for augmenting the blood supply of the scapular border or can be used to harvest the scapular angle as a separate osseous flap.
PATIENT HISTORY AND PHYSICAL FINDINGS
Determine if the patient has had previous head and neck surgery that would limit recipient vessel options or donor sites for microsurgical reconstruction.
Assess the patient’s level of function and which donor site will result in the least morbidity.
A scapular flap may be advantageous for older patients with compromised mobility who will have greater difficulty ambulating after surgery if a lower extremity donor site is chosen.1
Inspect the patient’s dental occlusion and determine whether any diseased dentition needs to be managed perioperatively and whether dental rehabilitation will be performed.2
IMAGING
Preoperative CT angiography may be useful to exclude lower extremity flap options such as the fibular flap in a patient with claudication and suspected peripheral vascular disease.
Virtual surgical planning may be helpful for complex head and neck reconstruction. A three-dimensional reconstruction of the recipient and scapula donor sites can be produced using CT imaging. Osteotomy sites at both the recipient and donor scapula locations may be planned preoperatively and a cutting jig developed to facilitate scapular contouring and inset.3
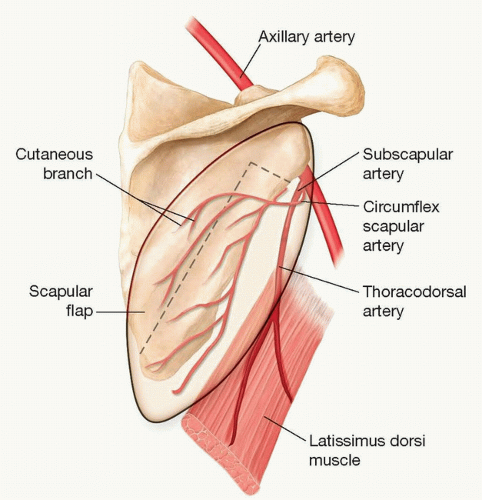 FIG 1 • Demonstration of the cutaneous branch of the circumflex scapular artery exiting the triangular fossa defined by the teres major, teres minor, and long head of triceps. The versatility of the scapular osteocutaneous flap relates to the multiple soft tissue elements including skin, fat, fascia, and the latissimus and serratus muscles that can be elevated with the flap based on the subscapular system. Additionally, the lateral scapular border is perfused by both the circumflex scapular and angular arteries, enabling separate bone flaps to be harvested. |
SURGICAL MANAGEMENT
The parascapular osteocutaneous flap is particularly useful for composite tissue defects with a large soft tissue component.
Multiple skin paddles and muscle flaps, including the latissimus and serratus, can be transferred with scapular bone based on the circumflex scapular artery,2,4 enabling reconstruction of some of the most complex three-dimensional defects.
This flap is unique among other choices used for mandibular reconstruction including fibula, iliac crest, and radial forearm free flaps, because the lateral scapular bone
is vascularized by a circumflex scapular pedicle branch independent from the branch supplying the skin paddle.
The bone can be inset into segmental defects of the mandible or used as a mandibular onlay, whereas the skin paddle can be safely rotated up to 180 degrees in relation to the bone.
Preoperative Planning
Determine the anticipated length of the bony deficit at the recipient site and whether a scapula flap will provide sufficient bone to reconstruct the defect.
Discuss with the patient and surgical team the functional goals of the reconstruction. Most male patients will be able to accommodate osteointegrated implants into their scapula flaps, although some female patients will have insufficient bone stock.5
Decide whether a two-team approach will be possible based on the positioning needs of the team working at the head and neck prior to transfer of the microsurgical free flap.
Positioning
The patient is placed in the supine position for induction of general anesthesia.
A bump is placed under the shoulder ipsilateral to the flap harvest site. This provides sufficient exposure of the upper back, and no beanbag is required for immobilization.
Following flap harvest, the bump may be removed, enabling a simple transfer to the supine position.

FIG 2 • A. The patient is positioned with a bump under the back on the side of flap harvest. The arm is elevated and will be suspended to a Z-arm that crosses the patient’s body. B. The goal of the setup is to minimize pressure on the forearm and avoid complications of neurapraxia and nerve palsy. A sterile Mayo stand cover is placed over the Z-arm and secured in place with two rolls of gauze. C. A sterile arm sleeve is placed over the arm after it has been sterilely prepared. D. The sleeve is secured to the arm with a gauze roll, and then, the gauze is secured to the Z-arm using two Kocher clamps. This strategy provides plenty of cushioning for the forearm without creating any areas of focal pressure that could result in nerve injury.
A Z-arm is placed on the side of the operating table opposite the back (FIG 2A). The patient’s arm will be suspended to this following sterile preparation and draping.
The arm ipsilateral to the flap harvest site is prepped and draped in addition to the upper back.
A Mayo stand cover is placed over the Z-arm, and this is wrapped with two rolls of gauze (FIG 2B).
A sleeve is placed over the prepped arm past the level of the elbow (FIG 2C). The sleeve is secured with a roll of gauze wrapped from the hand up.
Two Kocher clamps are then used to suspend the patient’s arm to the Z-arm (FIG 2D).
This technique avoids any areas of concentrated pressure on the arm and minimizes the risk of peripheral nerve injury.
The back is then draped with sterile towels and sheets.
Approach
The operative approach to raising the osteocutaneous parascapular flap depends upon the design of the skin paddle. We tend to design the skin paddle on the back along the axis of the arm so that the donor-site scar will be hidden under the arm. However, the skin paddle can be oriented in any direction around the triangular fossa.
Once the skin paddle has been designed, we approach flap elevation and pedicle identification by raising the flap from caudad to cephalad. However, the flap pedicle may also be approached by raising the skin paddle from its lateral or medial aspect.
TECHNIQUES
▪ Flap Elevation
Flap Design
Landmarks: lateral scapular border, teres major, teres minor, long head of triceps
The skin paddle of the flap is designed around the triangular fossa through which the circumflex scapular artery passes.
A depression superior to the teres major can usually be palpated and used to identify the triangular fossa (TECH FIG 1A).
The teres major measures two fingerbreadths wide and runs almost parallel to the lateral scapular border.
If the muscle cannot be palpated, then the lateral border of the scapula may be identified and traced just proximal to the glenohumeral joint.
The triangular fossa is located two fingerbreadths medial to this junction of the lateral scapular border and glenohumeral joint.
Confirmation can be performed with a pencil Doppler.
A skin paddle 5 to 10 cm in width and 16 to 46 cm in length can be harvested and enable primary closure (TECH FIG 1B).
Cadaver studies have demonstrated that branches of the circumflex scapular artery emerge radially from the triangular fossa and even perfuse the anterior chest wall at least as far as the anterior axillary line.6 The implication is that a long skin paddle can be harvested and followed into the inframammary fold to keep the donor site discrete.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree