| Enophthalmos caused by orbital floor resorption in silent sinus syndrome |
| Secondary volume augmentation after enucleation/evisceration or orbital fracture repair |
| History of orbital trauma, sinus disease, breast cancer or other malignancies |
| Exophthalmometry |
| Ocular ductions, cover/uncover testing |
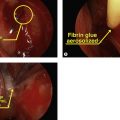
| Photographs documenting eye movements in nine fields and worm’s eye views |
| Examination by otolaryngology |
| CT scan of orbit and sinuses |
Introduction
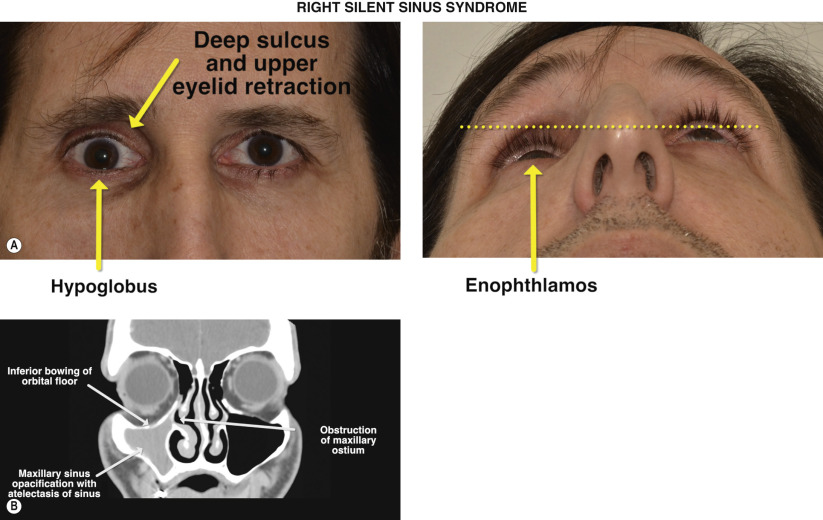
Silent sinus syndrome describes an indolent and chronic disease characterized by atelectasis of the maxillary sinus due to obstruction of the ostium. The resultant collapse of the maxillary sinus is associated with inferior bowing of the orbital floor that increases the effective orbital volume. Clinically, this is manifested by enophthalmos, hypoglobus, and a superior sulcus deformity. The condition is described as silent owing to little or no signs of sinusitis or nasal congestion.
Primary treatment is aimed towards aeration of the sinus by enlarging the native maxillary ostium with functional endoscopic sinus surgery. Microbial cultures of the sinus aspirate are typically sterile in nature and antimicrobial therapy has no role in the management of silent sinus syndrome. In a small percentage of patients who have underwent endoscopic sinus surgery alone, the orbital floor can re-expand, improving the enophthalmos but rarely to the pre-disease state. Treatment of the globe malposition is achieved by augmenting the orbital volume with alloplastic implants in a fashion similar to repair of an orbital fracture ( Chapter 67 ).
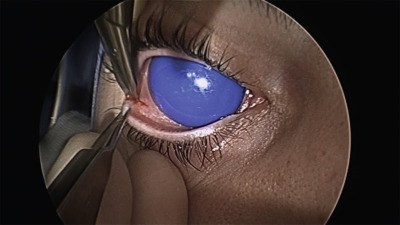
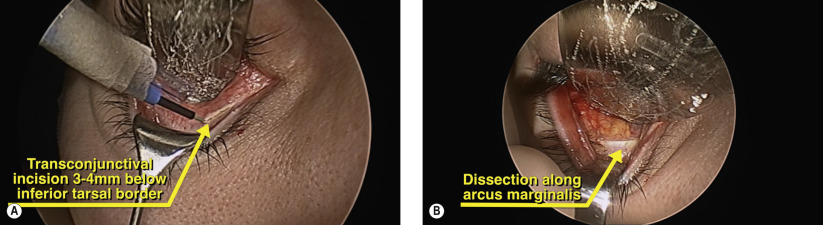
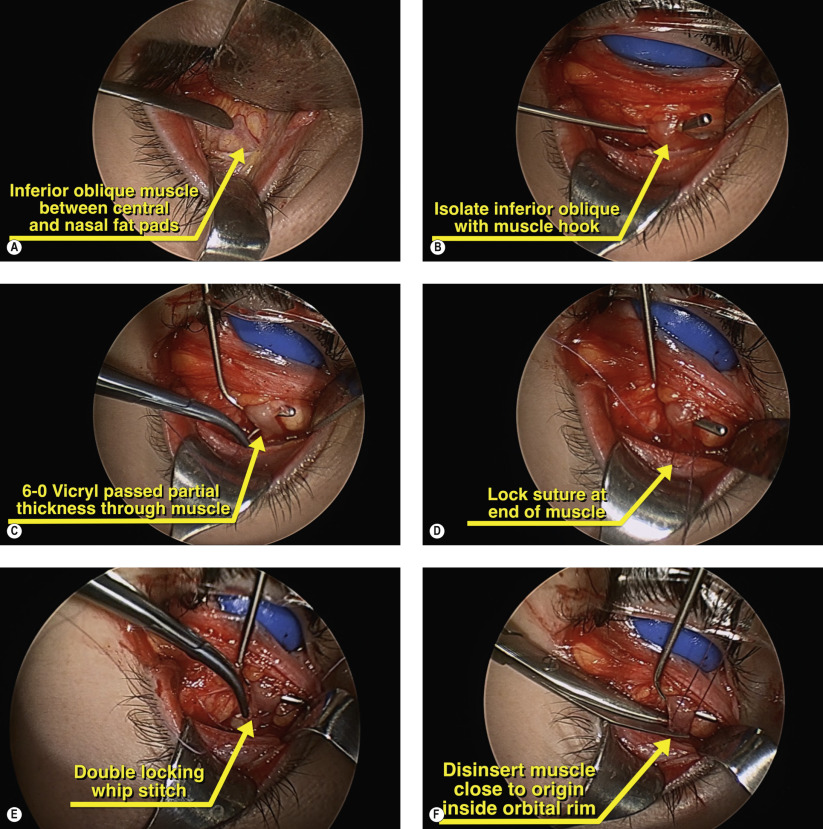
A variety of implants have been described, including autologous bone, porous polyethylene, hydroxyapatite, and titanium mesh. Our preference is to use a porous polyethylene enophthalmos wedge along the floor defect and covered by a thin barrier sheet of porous polyethylene with or without embedded titanium mesh. The surgery is carried out using a transconjunctival approach and can be performed simultaneously with endoscopic sinus surgery to address the maxillary sinus disease.
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


