| Vision-threatening papilledema refractory to maximal medical therapy |
| History of medication use associated with idiopathic intracranial hypertension (IIH) – oral contraceptives, antibiotics, chemotherapeutics, steroids, and acne medications |
| Dandy’s criteria for increased intracranial pressure (ICP) – headaches, nausea, vomiting, transient visual obscurations, papilledema, non-localizing unilateral or bilateral abducens palsy |
| Documentation of body habitus and gender |
| History of prior therapy for IIH – weight loss, carbonic anhydrase inhibitors, CSF shunts |
| Magnetic resonance imaging of the brain, orbits as well as MRA/MRV |
| Lumbar puncture with documentation of chemistries and opening pressure |
| Prior visual field testing if available |
Introduction
Optic nerve sheath fenestration (ONSF) is most commonly performed for vision-threatening papilledema associated with idiopathic intracranial hypertension (IIH). Other conditions where ONSF may be performed include optic nerve sheath hemorrhage, cryptococcal meningitis with papilledema, dural sinus thrombosis, and cancer-associated intracranial hypertensions with papilledema.
The work-up of papilledema associated with IIH first involves a detailed medication history to identify possible associations. Signs and symptoms of IIH should be elicited and documented. Automated visual field testing and optic nerve photographs should be obtained and then MR imaging is performed to rule out a mass effect causing the increased intracranial pressure (ICP) as well as vascular studies to rule out sinus thrombosis. Once imaging is deemed normal, attention is focused towards lumbar puncture to establish the opening pressure, which is elevated over 20 cm H 2 O in non-obese and over 25 cm H 2 O in obese patients. Infectious meningitis should be ruled out by normal chemistries and cultures if indicated.
Weight reduction and oral acetazolamide therapy is the mainstay of treatment for IIH. Patients with severe headaches are candidates for peritoneal shunts and should be referred to neurosurgery or interventional radiology. Vision-threatening papilledema is addressed by ONSF.
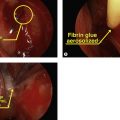
ONSF can be performed through a medial orbitotomy approach with disinsertion of the medial rectus, lateral orbitotomy with or without bone removal or through a superomedial eyelid crease incision. The latter technique is our preferred approach owing to its rapid, minimally invasive access to the medial optic nerve sheath. The surgery can be performed with a microscope or headlight and with optimal exposure can be performed under 30 minutes.
Surgical Technique

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


