INTRODUCTION
Open venous surgery still remains an important part of the treatment tool kit for patients with chronic venous insufficiency or lower-extremity varicose veins. Operative options include high ligation with division, with or without stripping of the great saphenous vein (GSV) or short saphenous vein (SSV). Open surgery is less frequent with the advent of endovascular intervention; however, the evolution of surgical techniques has made the current open surgical techniques much less invasive. This chapter provides an explanation of the indications and operative procedures for the ligation and stripping of superficial veins. Other saphenous sparing open surgical techniques include the CHIVA (cure conservatrice et hémodynamique de l’insuffisance veineuse en ambulatiore [ambulatory conservative hemodynamic management of varicose veins]), the ASVAL (ablation sélective des varices sous anesthésie locale [i.e., ambulatory selective varicose vein ablation under local anesthesia]) technique, and phlebectomy, which are described in Chapter 10.
Basic concepts: Venous anatomy, presentation, history, and physical examination, as well as diagnosis, have already been reviewed in Chapters 1–3 . Open surgical venous ligation (Trendelenburg procedure) was performed through a longer incision along the line of the GSV. This technique was subsequently modified by Moore and Homan; Keller, who utilized a smaller incision at the groin; Charles Mayo, who developed an external ring stripper for the removal of the GSV; and Babcock, who developed inversion vein stripping.
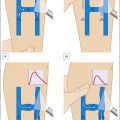
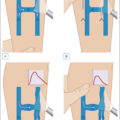
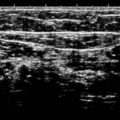
There are some specific considerations that are important to discuss when considering open surgery for superficial veins. Superficial veins are those that are located between the deep fascia and the skin. Specifically, the GSV originates from the median superficial veins on the dorsum of the foot. It follows a course in front of the medial malleolus along the medial border of the tibia, where it is closely associated with the saphenous nerve. Posterior and anterior accessory saphenous veins join the GSV in the calf and the thigh. In the calf, varicosities arising from the posterior accessory GSV may not connect with the mainstem of the GSV, draining instead to the posterior arch vein of Leonardo ( Fig. 12.1 ). More centrally, the GSV pierces the cribriform fascia at the fossa ovalis over the femoral triangle, where it joins the femoral vein. At the fossa ovalis, there are multiple named (superficial circumflex iliac, superficial epigastric, and external pudendal) and unnamed veins that drain into the GSV. The GSV has its own fascial covering; it lies in the superficial saphenous subcompartment, which can be identified on ultrasound as saphenous “eye” ( Fig. 12.2 ). This saphenous fascia is variable in its extent; the GSV may exit the fascia in the thigh or the calf but is sometimes continuous until the foot. In contrast, the saphenous tributaries run in a more superficial plane surrounded by adipose tissue and lack a fascial covering. This distinction can be of relevance in operative planning, for example, the GSV may require stripping, while more superficial varices may require phlebectomy. The saphenous vein has 4–25 valves, and the terminal and preterminal valve can usually be clearly identified on ultrasound ( Fig. 12.3 ). On ultrasound, attention is directed to the size of the saphenofemoral junction (SFJ), size of GSV, duration of reflux, as well as other features like superficial thrombophlebitis or vein wall calcification ( Fig. 12.4 ). The SSV originates from the lateral side of the foot and drains into the popliteal vein (see Fig. 12.1 ). The junction of the SSV into the popliteal vein may be variable, occurring 10 cm on either side of the crossing of a line perpendicular to the posterior knee joint line. The sural nerve lies in close proximity to the SSV, especially in the distal two-thirds of the calf. The SSV has 4–13 venous valves. The posterior intersaphenous thigh vein of Giacomini connects the GSV and SSV. Perforating veins connect the superficial to the deep system, are usually multiple, and are overall classified into thigh or calf perforators. Older terminology including greater, long, or lesser saphenous veins should not be used for proper documentation and uniform reporting standards.
Anatomy of the (A) great saphenous vein; (B) short saphenous vein; and (C) perforators. a , Artery; v , vein; n , nerve; SPC , superficial posterior compartment; PTV , paired tibial veins.
Ultrasound appearance of the great saphenous vein with the inset illustrating the appearance of the “saphenous eye.” GSV , Great saphenous vein.
Ultrasound image demonstrating an incompetent terminal valve at the saphenofemoral junction ( SFJ ) ( blue arrow ).
Ultrasound image demonstrating partial compressibility of the great saphenous vein ( GSV ) due to significant vein wall calcification ( blue arrow ).
Patients usually seek treatment for symptomatic varicose veins (being, pain, aching, heaviness, fatigue, pruritus, arms, tenderness along line of the vein, superficial thrombophlebitis); chronic venous insufficiency (edema, in changes including lipodermatosclerosis, eczema, pigmentation, atrophie blance, corona phlebectatica, healed or active ulceration); or cosmesis. General measures like the use of compression, hydration, avoiding prolonged periods of standing, ankle mobility exercises, and the role of medical management have been covered in Chapters 14 and 15.
Preoperative evaluation consists of a complete history and examination. Physical examination with the Trendelenburg test or segmental tourniquet application is not routinely performed but may be useful in certain patients to determine the optimal location of phlebectomy incisions. A bedside ultrasound performed by the surgeon is usually extremely useful to augment the information available from the preoperative duplex scan and aid in operative planning. This can identify specific anatomic concerns, like the location of a refluxing anterior saphenous vein, or mark the location of the saphenopopliteal junction. The patient is encouraged to point out specific varices that may be most concerning, and these can be screened with ultrasound preoperatively. Additional quality-of-life questionnaires and a clear discussion on the pathophysiology of the venous disease, preoperative imaging, and expected long-term and short-term symptomatic and cosmetic outcomes are performed and documented. Clinical pictures of the entire lower extremity, medial, lateral, and posterior with the patient standing, are obtained for the electronic medical record. Open venous surgery is performed as an outpatient procedure under local tumescent, spinal, or general anesthesia. Chemoprophylaxis for deep vein thrombosis (DVT) may be indicated in selective patients (obese, prior DVT, multiple risk factors for DVT).
Indications for Open Venous Surgery
Open venous surgery is indicated in patients with GSV size greater than 15 mm, an aneurysmal SFJ, severe vein wall calcification (risk of failure of endovenous modalities), large dilated vein located immediately under the skin (risk of skin burn), excessive tortuosity, previously resolved thrombophlebitis (inability to secure wire access for endovenous ablation), or residual or recurrent varicose veins with the failure of prior endovenous therapy. Other rare indications are progressive superficial thrombophlebitis to closer than 5 cm of the SFJ, despite anticoagulation or in patients who cannot be anticoagulated.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


