and Ziv Gil2
(1)
Division of Otolaryngology Head and Neck Surgery and Maxillofacial Surgery, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel
(2)
The Head and Neck Center Department of Otolaryngology Head and Neck Surgery, Rambam Healthcare Campus, Haifa, Israel
Keywords
Paranasal sinus malignancyMaxillofacial surgeryMaxillectomySurgical techniquesSquamous cell carcinomaOrbital exenterationReconstructionConventional open transfacial approaches involve various skin incisions and osteotomies of the maxillary, frontal, and ethmoidal bones. The exposure of the suprastructure of the maxilla involved lateral rhinotomy incision, whereas suprastructure maxillectomy and infrastructure maxillectomy are performed via Weber-Ferguson incisions. Lynch incision may be used to approach the frontal sinus lateral to the supraorbital nerve, where endoscopic resection is unfeasible. Lateral rhinotomy may be combined with a Lynch incision. A Dieffenbach incision combined with a lateral rhinotomy incision is used for tumors that extend to the infraorbital rim, lateral orbital wall, zygoma, and orbit.
This chapter describes the common transfacial incisions used alone or in combination for resections in the craniofacial area.
4.1 Preoperative Evaluation and Anesthesia
All patients scheduled for operation are evaluated preoperatively by a head and neck surgeon and an anesthesiologist. If a free flap is planned, a preoperative physical examination by a plastic surgeon is essential. Radiological evaluation includes axial and coronal CT scans and MRI of the head and neck. Broad-spectrum antibiotics are instituted perioperatively, usually including a second-generation cephalosporin and metronidazole. All operations are performed with the patient in the supine position.
4.2 Surgical Technique
4.2.1 Transfacial Approaches
Traditional transfacial open approaches utilize natural skin creases to access the maxillofacial region. These incisions include lateral rhinotomy or Weber-Ferguson incisions to access the maxillary region, Lynch incision to access the frontal sinus, and Dieffenbach incision and its modification to access the orbital region or malar eminence.
4.2.1.1 Lateral Rhinotomy Incision
In cases of malignant tumors originating in the nasal cavity and maxillary sinus without palatal invasion, the lateral rhinotomy approach is used. Similarly, benign tumors with anterior maxillary wall involvement are approached with the same incision. This approach allows wide exposure of the maxillary antrum, nasal cavity, ethmoidal sinuses, and sphenoid sinus.
The facial incision extends along the lateral border of the nose, approximately 1 cm lateral to the midline. It starts cephalad medial canthus and extends down through the skin crest bordering the nasal ala. It is continued toward the philtrum (Fig. 4.1). After marking, the skin is injected with lidocaine (0.06 %) and epinephrine (1:1,000,000) for hemostasis and hydrodissection purposes. Following the incision with a number 15 blade, the dissection continues with electrocautery. Skin flaps are elevated medially and laterally in the level of the periosteum with the aid of a Freer dissector. Care is taken not to injure the infraorbital nerve. If the tumor infiltrates the anterior wall of the maxilla, the skin flaps should be thinner, and the fibrofatty tissue and muscles are left on the maxillary bone, to be included in the specimen. The flaps can be developed laterally to the level of the maxillary tuberosity, inferiorly to the upper gingival sulcus, superiorly to the frontal sinus and infraorbital rim, and medially to the nasion and nasal septum. It is not always necessary to separate the upper ala of the nostril from the philtrum. The flaps are held with 2.0 skin stitches and fish hooks.

Fig. 4.1
Lateral rhinotomy incision
4.2.1.2 Dieffenbach and Subciliary Incisions
These incisions are used to approach tumors involving the infraorbital rim and zygomatic root. The incision can be extended medially up to the level of the medial canthus or inferiorly to be included in a lateral rhinotomy incision.
The classic Dieffenbach incision extends along the lower border of the eyelid, along a skin crest. The incision extends from the medial canthus to the lateral canthus. Later modifications of this incision include the subciliary incision, which is located just below the cilia of the eyelid or the midciliary incision, located halfway between the Dieffenbach and subciliary incisions (Fig. 4.2).
Following the incision with a number 15 blade, the dissection continues with electrocautery. Skin flaps are elevated in superior and inferior directions in the level of the periosteum with the aid of a Freer dissector (Fig. 4.2). The superior border of the flap is the infraorbital rim and orbit and its inferior border is the anterior maxillary wall. Laterally it is extended to expose the maxillary tuberosity and the root of the zygoma, and medially it extends to the nasal bone. In elderly patients and those with previous irradiation, the redundant skin and subcutaneous tissue of the lower eyelid tends to swell, as the incision may compromise lymphatic drainage of this area. The skin in this area is closed with subcutaneous continuous number 5.0 prolene stitches, to prevent contractions of the thin skin in this area.

Fig. 4.2
Dieffenbach (left) and subciliary (right) incisions
4.2.1.3 Combined Lateral Rhinotomy and Dieffenbach Incisions
For tumors that extend from the nasal cavity and maxillary sinus to the malar eminence or root of the zygoma, an extension of the lateral rhinotomy is indicated. In such a case, the lateral rhinotomy incision is combined with a Dieffenbach incision, as shown in Fig. 4.3. The infraorbital rim should be preserved as much as possible, to prevent enophthalmos.
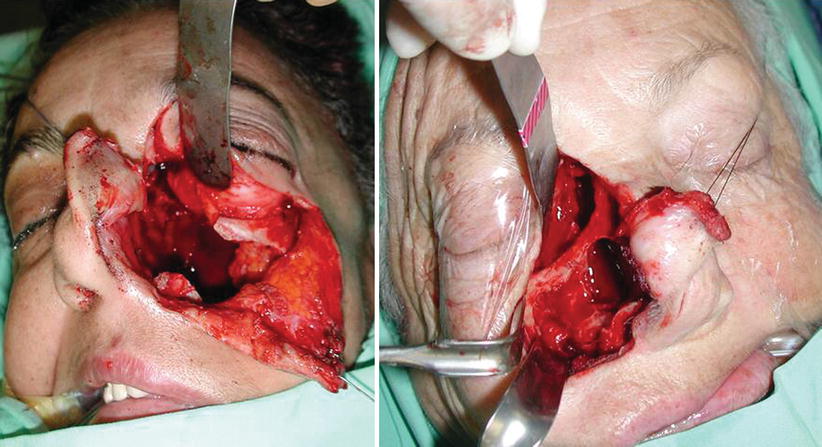
Fig. 4.3
Combined lateral rhinotomy and Lynch incision (right) and combined lateral rhinotomy and Dieffenbach incision (left)
4.2.1.4 Weber-Ferguson Incision
In cases of malignant tumors infiltrating the lateral maxillary wall or palate, total maxillectomy is performed via Weber-Ferguson incision. This incision allows exposure of the superior and inferior aspects of the maxilla and its complete en bloc resection. The facial incision begins as a lateral rhinotomy incision, which is continued toward the philtrum and extended down to the lip in the midline (Figs. 4.4, 4.5, 4.6, and 4.7). Inferiorly the incision continues along the gingivobuccal sulcus, extending laterally up to the retromolar area.

Fig. 4.4
A Weber-Ferguson incision begins as a lateral rhinotomy incision, which is extended to the lip in the midline
After marking, the skin and gingivobuccal sulcus are injected with lidocaine (0.06 %) and epinephrine (1:1,000,000) for hemostasis and hydrodissection purposes. Following the incision with a number 15 blade, the dissection continues with electrocautery. Skin flaps are elevated medially and laterally in the level of the periosteum as described above.
A unilateral gingivolabial incision is now made, extending up to the lateral buttress of the maxillary. The soft tissue of the cheek is raised from the anterior surface of the maxilla, transecting the infraorbital nerves and vessels if the superior and lateral walls of the maxilla must be approached. An upper cheek flap is developed laterally and superiorly up to the level of the inferior orbital rim and the maxillary tuberosity (Figs. 4.5, 4.6, and 4.7). Inferiorly, it can reach the pterygopalatine fossa.


Fig. 4.5
Elevation of an upper cheek flap (I)
Fig. 4.6
Elevation of an upper cheek flap (II)
Fig. 4.7
Tumor exposure and lower mucosal incision for partial maxillectomy. Note the osteotomy lines on the palate
4.2.1.5 Lynch Incision
The Lynch incision is used to approach tumors involving the frontal sinus. It can be extended laterally up to the level of the lateral canthus or inferiorly to be included in a lateral rhinotomy incision. The facial incision extends along the lower border of the eyebrow, allowing it to be concealed at the hair-skin junction. If the incision is made inside the eyebrow, a thick scar may be noticed, giving inferior cosmetic results. The incision is extended down, approximately half a centimeter medial to the medial canthus.
Following the incision with a number 15 blade, the dissection continues with electrocautery. Skin flaps are elevated in superior and inferior directions at the level of the periosteum, with the aid of a Freer dissector. The superior border of the flap is the frontal bone and glabella. Its inferior border is the superior orbital rim and the roof of the orbit; within its medial border lies the lacrimal fossa, with its duct and sac, and lateral border is the root of the zygoma. A Lynch incision can be an extension of a lateral rhinotomy incision.
4.2.2 Transfacial Subtotal Maxillectomy
Partial maxillectomies may be performed transorally or through a transfacial approach. After performing the Weber-Ferguson incision, the anterior maxillary wall is widely exposed (Figs. 4.4, 4.5, and 4.6). The infraorbital nerve is identified and preserved if possible. The bone is inspected carefully to identify its integrity and areas of tumor infiltration (Fig. 4.7). The mucosa is first incised with monopolar cautery. Osteotomies along the anterior, inferior, and medial walls of the maxilla are now performed with a motorized reciprocating saw. The lines of the osteotomies are the fossa canina (above the dental roots) as the inferior border; the orbit, superior; the malar eminence, lateral; and the nasal cavity, medial (Fig. 4.8). The medial wall and part of the anterior wall of the maxilla are now retracted anteriorly with a Babcock grasper, and the tumor is freed from its attachments with a Mayo scissors and Freer elevator. If necessary, the rest of the tissue is extirpated with a Kerrison rongeur. Hemostasis is performed with warm saline irrigation. The cavity is inspected and hemostasis is completed with bipolar electrocautery. In most cases, branches of the sphenopalatine artery can be identified at the posterior wall of the maxilla lateral and superior to the choana. These are clamped with medium-size clips to prevent further bleeding. The maxillary defect is reconstructed with an artificial implant during surgery (Figs. 4.9 and 4.10).
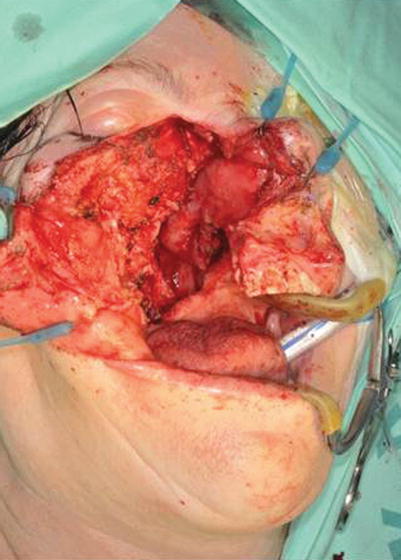


Fig. 4.8
The surgical field following tumor removal
Fig. 4.9
Reconstruction of the palate is performed with an obturator
Fig. 4.10
The Weber-Ferguson incision is closed with 5.0 nylon sutures
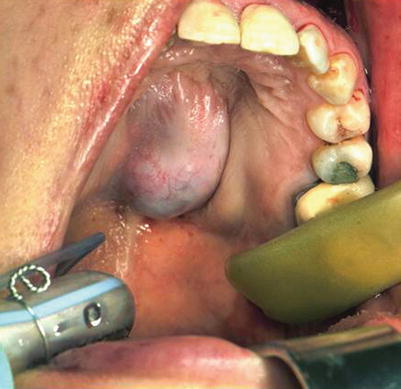
4.2.3 Midfacial Degloving Approach
This approach, which leaves no incisions and scars on the face, may be used in cases of tumors involving the midface and midpalate like the tumor shown in Fig. 4.11. Midfacial degloving can be approached through the mouth or by a combined transoral midfacial degloving approach. The operation starts with an incision of the mucosa at the gingivobuccal sulcus, approximately 5 mm above the teeth from first molar to first molar. Next, a complete transfixion incision is made and connected bilaterally with a complete intercartilaginous incision. This incision separates the upper lateral cartilages from the lower lateral cartilages. The upper lateral cartilages are left attached to the nasal frame and septal cartilage, and the lower lateral cartilages are included with the superiorly retracted flap. The procedure continues with undermining through the intercartilaginous incision over the face of the anterior maxillary sinus and superiorly over the frontal bone, releasing the soft tissue envelope from the nasal skeleton and nasal septal angle. The intercartilaginous incision is then continued caudally and medially through the periosteum of the nasal floor and pyriform aperture and connected to the transfixion incision (Fig. 4.12). A “degloving” of the facial soft tissues from the nasal skeleton and maxilla is now performed. The flap is held by placing a Penrose drain through each nostril and around the upper lip. Next, osteotomy of the anterior maxillary wall is performed ipsilaterally or bilaterally (Fig. 4.13). An incision is now performed around the tumor perorally (Fig. 4.14). The tumor is removed en bloc with the use of a fine osteotome and Mayo scissors, and the site is reconstructed with an obturator (Fig. 4.15).