and Ziv Gil2
(1)
Division of Otolaryngology Head and Neck Surgery and Maxillofacial Surgery, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel
(2)
The Head and Neck Center Department of Otolaryngology Head and Neck Surgery, Rambam Healthcare Campus, Haifa, Israel
Keywords
Infratemporal fossaTransfacialCraniofacialEndoscopic assistedOrbitozygomaticTransorbitalFar lateral approach11.1 Introduction
The classic open approaches to the skull base include the subcranial/subfrontal, orbitozygomatic, pterional, transpetrosal, middle fossa, retrosigmoid, and far lateral approaches. These approaches cover the anterior, middle, and posterior skull base from above (Fig. 11.1). Although these approaches permit tumor resection in most cases, there are still situations in which the inferior, lateral, or posterior aspects of the tumor are not adequately exposed by an individual approach. These include malignant or benign neoplasms with extensions to the maxillary antrum and palate caudally; to the cavernous sinus posteriorly; to the orbital apex, pterygopalatine fossa, or the infratemporal fossa laterally; or involvement of the nasopharynx and inferior aspect of the clivus inferoposteriorly. Such cases require a combination of several approaches in a single-stage procedure. In these combined approaches, a second approach, such as midfacial degloving or an orbitozygomatic, transfacial, endoscopic, or transorbital approach, is added to enable proper exposure and tumor extirpation. These combined approaches require additional incisions and osteotomies, depending on the type and extent of the tumor. This chapter describes combinations of the anterior and lateral approach frequently used for extirpation of complex tumors extending out from the anterior skull base.
Fig. 11.1
Classic open approaches to the skull base
11.2 Surgical Technique
For tumors that involve multiple compartments, especially tumors that invade the anterior and lateral skull base from other regions, there is a need to combine one or more approaches.
11.2.1 Combined Transorbital–Transcervical–Infratemporal Fossa Approach
A lateral skull base approach can be combined with a transcervical approach for tumors involving the parapharyngeal space, with transparotid approaches for tumors that extend below the infratemporal fossa (ITF), and with transfacial approaches for tumors that extend anteriorly. When the tumor extends to the orbit, paranasal sinuses, and anterior skull base, a combination with a standard transfacial approach may be required. In Fig. 11.2, a squamous cell carcinoma of the skin invading the orbit and paranasal sinuses required modification of the standard incision to achieve en bloc tumor resection. A combined ITF–transorbital approach was performed via a circular skin incision that included the superior and inferior orbital rims and the skin of the lids. The operation continues with total parotidectomy with sacrifice of the upper division of the facial nerve (Fig. 11.3). This is followed by segmental mandibulectomy and exposure of the root of the zygoma (Fig. 11.4), and then radial orbital exenteration (with the upper and lower lids) along with partial suprastructure maxillectomy to define the medial margin of the resection (Fig. 11.5). The extirpation of the tumor is completed with composite resection of the skin, zygomatic bone and arch, and the lateral orbital wall along with the orbital contents and maxilla (Fig. 11.6). Figures 11.7 and 11.8 show the surgical defect before and after reconstruction.


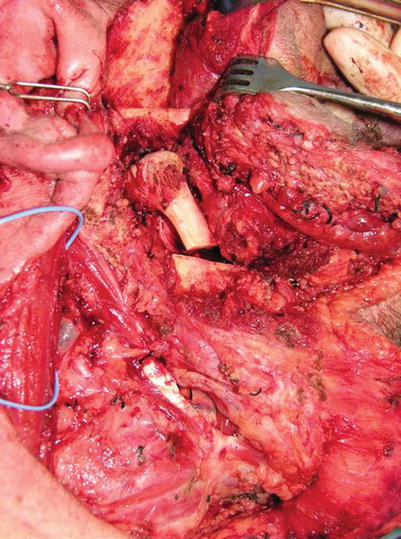




Fig. 11.2
A combined infratemporal fossa (ITF)–transorbital approach requiring modification of the standard incision
Fig. 11.3
Total parotidectomy and sacrifice of the upper division of the facial nerve
Fig. 11.4
Segmental mandibulectomy and exposure of the root of the zygoma
Fig. 11.5
Orbital exenteration, along with partial suprastructure maxillectomy
Fig. 11.6
Composite resection of the skin, zygomatic bone and arch, the lateral orbital wall, the orbital contents, and maxilla completes extirpation of the tumor
Fig. 11.7
The surgical defect before reconstruction
Fig. 11.8
The surgical defect after reconstruction
11.2.2 Combined Transfascial–Transorbital–Pterional Approach
For tumors that originate in the paranasal sinuses and invade the lateral skull base and orbit, the upper and lower lids often can be preserved. In such cases, the question mark incision is extended with a coronal incision, and the maxilla and orbit are approached via a lateral rhinotomy or Weber–Fergusson incisions (Fig. 11.9). The pterional or ITF approach is performed as described in Chap. 6, and the standard frontal osteotomy may be extended to include a portion of the orbital roof (Fig. 11.10). The specimen is combined with total maxillectomy and orbit exenteration (Fig. 11.11). Figures 11.12 and 11.13 show the superior and inferior margins of the resection after tumor removal. Figure 11.14 shows the specimen, which was resected en bloc with free margins. Reconstruction of the orbit and palate was achieved with anterolateral thigh free flap (Fig. 11.15).

Fig. 11.9




To preserve the upper and lower lids, the maxilla and orbit are approached via a lateral rhinotomy or Weber–Fergusson incisions
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
