Fig. 12.1
Longitudinal nail biopsy of an onychomycotic nail. The nail plate of the matrix and proximal nail bed is dystrophic showing an irregular, fragmented, and lifted surface with mounds of parakeratosis
The fungal hyphae on HE routinely stained sections are difficult to visualize; therefore, special fungi stains are needed to highlight its presence; these classically include periodic acid-Schiff (PAS) and Grocott methenamine silver (GMS). PAS technique works by exposing tissue to periodic acid, which oxidizes hydroxyl groups of cell wall polysaccharides into dialdehydes; the latter react with Schiff reagent, forming a magenta compound. The background is a faint pink, while fungi cell membranes stain a magenta-red color. In GMS stain, chromic acid is used to oxidize the hydroxyl groups forming aldehydes, which then react with the silver nitrate reducing it to metallic silver, making them visible. The slide has a light green background, while the hyphae are stained dark brown to black [1].
For a while, GMS was thought to be superior to PAS staining for finding fungal structures in biopsies; however, after several conducted studies, they concluded the deeper levels were increasing the detection of the fungi, rather than the stain used. Although no significant differences were reported between these two, PAS was found to be a more cost-effective stain [1, 2, 12].
Although the fungi structures are well visualized with the special stains described, histological examination does not allow the precise identification of the infecting agent; however, it can suggest the implicated pathogen by analyzing their morphology.
Usually, a dermatophytic infection is suspected when regular, septate hyphae running parallel to the nail surface are observed (Fig. 12.2).
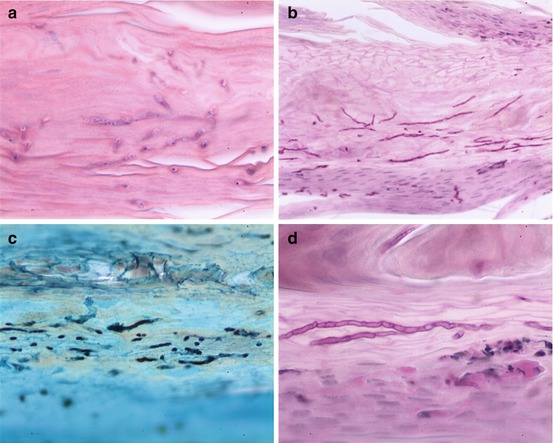
Fig. 12.2
Histological examination of dermatophytic onychomycosis. (a) H&E stain showing translucent hyphae spreading between corneocytes. (b) PAS stain highlighting hyphae in red-magenta color. These are regular and parallel-oriented to the nail surface. (c) Hyphae dyed in black with Grocott methenamine silver stain. (d) PAS stain showing regular, branching, septate hyphae
Yeasts are suspected when small round spores, some even budding, pseudohyphae, and short filaments are found. Spores without pseudohyphae can be contaminants (Fig. 12.3).
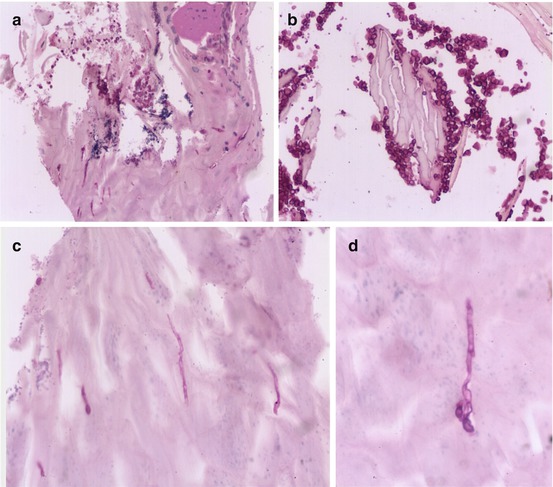
Fig. 12.3
Candida onychomycosis on a histological section stained with H&E. (a) Dystrophic nail plate with parakeratosis, plasma, bacterial colonies, and red-magenta dyed spores. (b) Multiple small round spores admixed with keratin. (c, d) Short and thin filaments and pseudohyphae, vertically oriented to the nail plate, are also found
NDM can display truncated spores with vertically thin arising perforating hyphae.
Although the former are the main causative onychomycosis agents, other ND fungi have been reported to cause infection like Aspergillus spp., Alternaria spp., Scopulariopsis brevicaulis, Emericella quadrilineata, and other microorganisms like Prototheca spp., and also Medlar bodies have been found in a case of melanonychia [13–17].
An uncommon and unique clinical presentation of onychomycosis caused by dermatophytes, also known as dermatophytoma, typically presents as a yellow longitudinal band or yellow or white patch. Histologically a dense mass of hyphae is found [10].
Punch samples of nail plate and nail bed or longitudinal nail biopsies are rarely performed, except when other inflammatory diseases are clinically suspected. When these are taken, the histological picture displays subungual hyperkeratosis with mounds of parakeratosis or foci of neutrophils, psoriasiform dermatitis with hyperplasia of the nail bed epithelium, and variable spongiosis with neutrophil exocytosis. In the absence of onychomycosis, another nail disorder can be recalled like psoriasis, lichen planus, or even a hematoma. Psoriasis can be difficult to differentiate from onychomycosis clinically and histopathologically [5].
KOH has a sensitivity between 53 and 76 % and mycological culture between 35 and 53 %; both tend to be sample dependent; nevertheless, the latter can identify the fungal species and sensitivities to antifungals but requires long incubation periods to yield a diagnosis. PAS-stained sections of nail clippings have the highest reported sensitivity, varying between 75 and 92 % according to different studies, and therefore are considered the gold standard diagnostic technique. It is the least likely to be affected by sampling methods and is also considered the most sensitive to monitor residual infection after adequate antifungal treatment. Combining these techniques has established decreased chances of false negatives; PAS staining combined with KOH reported sensitivities between 89 and 99.4 %, while PAS with culture gave between 93 and 96 %; however, PAS alone was better than the combination of KOH direct microscopy and culture with a sensitivity of 88.8 %. Hence, combination of PAS-stained nail clippings with either KOH or culture can give higher values of sensitivity and negative predictive values [4, 11, 18].
Although histopathology is a relatively fast diagnostic test, the nail needs to be fixed, dehydrated, embedded in paraffin, and sectioned before being stained [3]. A nail biopsy can be technically harder to process than a routine cutaneous specimen because of the hard keratin in the nail plate, so pretreatment with softening agents is needed to obtain high-quality sections. Useful softener agents described include potassium hydroxide (KOH), 4 % phenol, 5 % trichloroacetic acid in 10 % formalin, cider oil, chitin softening agent with mercuric chloride containing solutions, and more recently sodium hydroxide (NaOH), which has reported an improved ease of sectioning and adherence to slides, although fainter PAS staining and damage to melanin and hemosiderin pigments have been reported [10, 19].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


