© Springer International Publishing Switzerland 2017
Antonella Tosti, Tracey C. Vlahovic and Roberto Arenas (eds.)Onychomycosis10.1007/978-3-319-44853-4_1919. The Podiatric Approach
(1)
Department of Podiatric Medicine, Temple University School of Podiatric Medicine, 148 N 8th St, Philadelphia, 19107, PA, USA
Podiatric physicians have a unique practice situation, as they generally manage onychomycosis cases on a daily basis and in a specialized population (diabetes, Chap. 17). However, toenail disease may be caused by a variety of issues that are specifically foot related and not fungal related: trauma from shoes, biomechanical issues and forces, and infection compounded by shoe gear and adjacent skin conditions to the nails (i.e., interdigital tinea pedis). It is important when discussing the management and treatment of toenail onychomycosis that the visually similar biomechanical causes of nail dystrophy are also mentioned.
Patients commonly present to a podiatric physician’s office for the care of toenail pain (both infectious and noninfectious causes), discoloration that is cosmetically displeasing, and/or thickness that creates pressure in shoes. Patients are often under the belief that their nail presentation may be the result of a fungal infection; however, it is imperative that other factors on and around the nail unit are considered: biomechanics and shoe gear. These are unique to the toenail when compared to the fingernail. Biomechanics describes both the non-pathological and pathological forces involved in the gait cycle. The pathologic forces may result in digital deformities, soft tissue lesions (i.e., corns and calluses), bunions, arch and heel pain, and even skin breakdown (especially in a neuropathic patient). Both in the diabetic neuropathic population and those with painful or biomechanical issues, the podiatric practitioner will likely perform a biomechanical evaluation which includes gait analysis and function of the major joints of the foot and ankle.
Evaluating the Podiatric Patient
To evaluate a patient presenting with toenail onychomycosis, the practitioner should begin with completing a thorough history and physical evaluation. With treatment options ranging from systemic to surgical, knowledge of medical history, current medications, and family history will aid differential diagnosis and treatment plan. Key questions include how long have you had the nail changes, is it painful, and has it affected your quality of life? Is the patient able to bend and visualize the nails in order to trim them? Daily shoe gear choices, work and athletic activities, and home and work environment will all assist treatment plan selection. Level of immunosuppression, pedal vascular status, and ability to take oral or apply topical medication should be taken into account. Discussion and examination of any other skin rashes or conditions should be completed, as psoriasis and eczema can mimic mycotic toenails.
Visual assessment is imperative. Since the Zaias classification was proposed in 1972, modifications have been proposed and published to reflect the wide array of dermatophytes, non-dermatophyte molds, and yeasts as well as the complications of various patterns occurring in the same nail or other inflammatory diseases co-presenting with mycosis [1]. Nail plate changes include:
DLSO where the invasion begins at the hyponychium and disturbs the distal nail bed
Proximal subungual onychomycosis (PSO) where invasion begins proximally
Superficial white onychomycosis (SWO) where the upper surface of the nail plate is first attacked [1]
Total dystrophic which describes total nail plate involvement and surrounding periungual tissue
Endonyx onychomycosis (EO) which describes distal nail plate attack resulting in a deeper penetration of hyphae
In addition, the physician should determine how many toenails are involved on one or both feet, percent involvement of the nail, any biomechanically aggravating factors that could contribute to nail dystrophy (adductovarus fifth digit, hammertoe, or hallux valgus), and the presence of tinea pedis interdigitally or plantarly.
Approximately 50 % of nail disease is caused by onychomycosis [2]; the remainder conditions mimic onychomycosis, having similar signs and symptoms including psoriasis, lichen planus, reactive arthritis, allergic/irritant contact dermatitis, and eczema. Other differential diagnoses include alopecia, nail changes secondary to biomechanical issues, melanoma (and other skin cancers), traumatic onycholysis, 20-nail dystrophy, and pachyonychia [3–5].
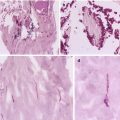
Since not all presenting nail disease is mycotic, it is important to confirm with laboratory diagnosis if the treatment plan includes oral antifungal therapy, if there is concomitant skin disease difficult to distinguish in the nails, and if the patient has been on antifungal therapy previously and disease has recurred. Laboratory diagnostic methods include direct microscopy (KOH test), nail plate biopsy for periodic acid-Schiff (PAS) stain, and fungal culture. Generally, KOH and fungal culture are done together; KOH shows the presence of hyphae and cultures the species present. Unfortunately, fungal cultivation is a slow process (up to 4 weeks) and may generate false-negative results in 40 % of the cases that are microscopically positive [6]. An alternative PAS involves sending nail plate (commonly referred to as, but not a true biopsy) for staining to determine presence of dermatophytes. PAS provides quicker results and is more sensitive, while culture is the more specific (regarding species) [7–9].
Standard mycological tests, KOH and fungal culture, may yield false-negative or false-positive results, and require time to verify the pathogens [10]. Accurate diagnoses are often delayed due to lack of both specific and rapid methods of pathogen identification. When the mycological analyses are negative and clinical picture highly suggestive of onychomycosis, polymerase chain reaction (PCR) testing may be an option [11]. Antifungal drug efficacy and dosages may differ for different causative pathogens, and it has been hypothesized that mixed and non-dermatophyte onychomycosis may be cause for high rate of treatment failures [12]. A rapidly sensitive method for detection and identification will better guide an appropriate treatment strategy. PCR detects a specific DNA sequence; moreover, fungi species-specific PCR diagnostic methods are available deepening our understanding and treatment of onychomycosis [13–15]. Since DNA is extremely resistant and can persist even in the absence of viable hyphae, DNA amplification techniques such as PCR may represent a useful addition to standard procedure [16]. Time will tell how truly beneficial PCR will be both in the physician office and in clinical trials.
Podiatric Nail Issues
Toenail Onychomycosis
Onychomycosis or tinea unguium is caused by invasion of the nail unit by dermatophytes, non-dermatophyte molds, and/or Candida albicans. Toenails subject to trauma from either a biomechanical reason or otherwise may be the first to present. For example, a limitation in plantarflexory motion of the first metatarsophalangeal joint may predispose the hallux nail to trauma against the toe box of the shoe, thus allowing dermatophyte invasion to take place. In addition to nail trauma as a harbinger of mycosis, tinea pedis or tinea cruris on the patient may be concomitantly found and be a source of infection. When a patient presents with mycotic toenails, it is useful not only to inspect interdigitally and plantarly for signs of tinea pedis but also to ask if they have any scaly rashes elsewhere on the body or past use of a topical antifungal anywhere else on the body.
Podiatric practitioners recommend the oral and topical medications and laser procedures that have been covered in this book (Chaps 19, 20, and 21). Some podiatric physicians recommend in-office-dispensed, over-the-counter, and compounded topical remedies as a convenience and cost-saving entity to the patients; however, these are not specifically FDA approved for mycotic toenails. Also, topical urea preparations have classically been used to soften, thin, and smooth the nail plate both before and during topical antifungal therapy but have not been specifically studied in a clinical trial.
One of the most common podiatric in-office procedures, nail debridement, is defined as the mechanical reduction of toenail length and thickness using nail nipper or rotating burr (such as a Dremel device). Nail debridement may provide a valuable adjunct for patients experiencing pain upon ambulation and in shoe gear [17]. While debridement alone improves quality of life and nail thickness, it does not result in mycological cure [18]. In one study, the concomitant use of topical ciclopirox and debridement improved a patient’s quality of life and resulted in mycologic cure [18]. However, debridement added to oral antifungal therapy may offer a only a small benefit [19, 20]. Debridement can provide pain relief and improved patient satisfaction, affording an opportunity to encourage adherence. It may offer benefits through reduced fungal load and enhanced penetration of topical drugs into the nail unit. For patients who opt against pharmacological treatment, debridement will allow more comfort in shoe gear and reduce potential pressure on the nail bed, especially if diabetic neuropathy is present. In the diabetic patient who is compromised both vascularly and neurologically, mycotic nail debridement is routinely performed by a podiatric practitioner every 9–12 weeks in order to decrease pressure and complications that may arise from the thickness of nails and prevent the patient from creating a problematic situation by performing self-care of the nails.
Nail avulsion, a procedure that creates separation of the nail plate from the nail bed, can be achieved nonsurgically with daily application of topical 40 % urea for 1–2 weeks [21]. Generally, this is followed by application of a topical antifungal once the toenail has been removed, repeating as necessary. It is more common in Europe [21]. Chemical nail avulsion can be useful in patients who have a needle/procedure phobia, who have peripheral vascular disease or another comorbidity precluding pharmacological intervention, or have a single nail infected. However, removal of the nail itself will not result in clearance of the infection, even followed by topical antifungal therapy.
For a singularly painful or thickened nail, some patients may opt for a surgical total nail removal. Surgery involves application of local anesthesia to the digit followed by removal of the nail plate in toto. Simple total avulsion of the nail itself is not curative for a mycotic nail; as the procedure has not addressed the basis of infection. Combining nail avulsion and topical antifungals has been described as the preferred treatment plan. Total nail avulsion with the use of a topical azole cream applied twice daily to the exposed nail bed resulted in a high dropout rate. All patients with total dystrophic onychomycosis failed, and only 56 % patients (15/27) were cured with this approach suggesting that the procedure should not be generally suggested for the treatment of onychomycosis [22].
Nail avulsion has been suggested to obtain a better specimen for fungal culture but should only be used in situations where both systemic and topical antifungal therapies have failed [21]. Contraindications include patients with peripheral vascular disease, autoimmune disorders, collagen vascular disease, diabetes, hemostasis disorders, and acute infection/inflammation of the periungual tissue [23]. Possible keratinization of the nail bed as the nail plate is growing is also a concern, thus creating a “disappearing nail bed” scenario where the nail plate will never adhere to the nail bed [24].
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


