Chapter 7 Nonoperative Management of Anterior Cruciate Ligament Deficient Patients
Anterior Cruciate Ligament Deficiency: The Need for Muscle Strengthening
The knee joint’s location in the middle of the lower limb kinetic chain is imposed to high loads, which reach multiple the body mass, particularly in the single stance phase of sport activities.1,2 Rupture of the anterior cruciate ligament (ACL) destabilizes the knee joint,3–5 thus making ACL deficient knees prone to repeated subluxations, which form a potential cause for secondary damage to the joint.6–8 Subsequently, dynamic stabilization through the quadriceps and hamstrings becomes very crucial for the protection of the injured knee.9,10 Apart from its mechanical role, the ACL functions as a sensory organ due to the mechanoreceptors within its substance.11 After its rupture, this function is lost, and therefore optimization of the lower limb muscle properties becomes increasingly important in order to compensate for the resulting anterior and rotational knee instability.
Exercise in ACL deficient patients aims at the improvement of various aspects of muscle properties including reflexes, strength, endurance, and coordination with other muscles. Functional exercise that reeducates the neuromuscular coordination holds the central role in rehabilitation programs, as growing evidence supports the development of preprogrammed compensatory muscle activation strategies for efficient shear force dissipation during injured knee loading.12–16 However, the fundamental issue of the need for strength testing and the value of strengthening exercises still leaves room for investigation.
Among the criteria for progression of ACL rehabilitation is the level of quadriceps and hamstring weakness.17,18 Strength testing and exercise have been traditionally incorporated into musculoskeletal rehabilitation regimens. Although the connection between the level of quadriceps strength and functional status has been disputed,19–22 some studies support the interrelation between functional performance of the knee and thigh muscle strength. It is of clinical importance for ACL rehabilitation that patients with greater than normal strength in the injured limb seem to reduce abnormalities during low- and high-stress activities.23 Quadriceps strength appears to determine the functional ability of the ACL deficient or operated limb to a great degree.24,25 Its weakness coincides with low functional performance26 and pathological gait pattern.27 In addition, functional improvement in ACL deficient athletes after training followed the same pattern as the strength of both the quadriceps and hamstrings.23,28
Likewise, increase in hamstring strength after functional exercise incorporating strengthening, stretching, and plyometric drills paralleled a decrease in peak landing forces, and hence safer landing.29 Hamstring strength has also been associated with the level of knee function10,30 and performance,31 and increasing the hamstring–quadriceps (H:Q) strength ratio has be come a rule in order to promote dynamic control of the ACL deficient knee.32,33 Even more, this improvement has been connected with the return to physical activity after ACL injury,34 and the strength of both thigh muscle groups reflects the functional improvement23,28 and the ability to return to physical activity.34
It appears that changes in muscle strength might be a global reflection of muscle properties, including neural changes.35 It seems that adequate strength ensures that a solid basis is built for other refined neuromuscular properties. In other words, adequate strength secures the proper background for the development of global muscle properties. Therefore, it appears that objective evaluation of strength has a valuable position in the functional assessment after ACL injury, and in combination with our findings, it could be suggested that therapeutic intervention should minimize strength weakness, which persists over time when not addressed.
Importance of the Hamstrings, Especially in Soccer Players: Our Research
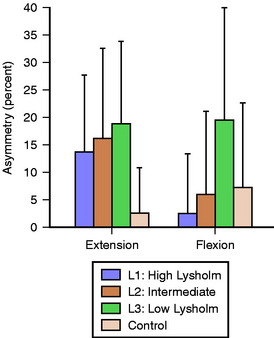
The first study focused on revealing a possible connection of quadriceps and hamstring strength deficits with the level of knee function determined by Lysholm score.30 Three groups of ACL deficient amateur soccer players were examined at different levels of knee function and were compared with a group of controls matched for the preinjury level of activity. The median Lysholm scores of the low, intermediate, and high knee functioning groups were 64.5, 76, and 86 points, respectively. Weakness depicted by the contrast to the healthy condition was significant in all cases and ranged from 19% to 35% according to the muscle or the patient group. Regarding the side-to-side deficit, these major muscle groups did not follow the same pattern. The strength asymmetry of the quadriceps was consistently significant even in the high functioning knees, being greater than 14%, in contrast to the hamstrings, which revealed acceptable symmetry within the normal levels (about 2% to less than 6%) at the high and intermediate knee function groups. Only the poorly functioning athletes had a significant 19% deficit (Fig. 7-1), which places hamstring strength asymmetry (H asymmetry) as a discriminating factor for knee functionality.
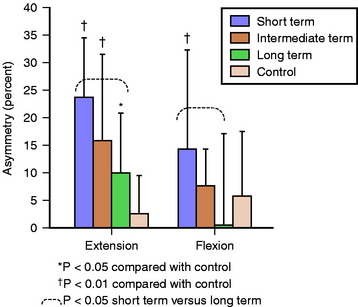
The importance of assessing H asymmetry is highlighted in our recent study that examined different groups of amateur athletes involved in cutting and twisting sports such as soccer, basketball, and handball at different times since ACL rupture.36 We tested the quadriceps and hamstring strength of 36 patients with unilateral ACL deficiency who were divided into three equal groups with mean times for chronicity of about 4, 11, and 57 months for short term, intermediate term, and long term, respectively. We investigated how the strength weakness evolved with time, using the strength of matched healthy controls as a baseline score. Additionally, we questioned whether the quadriceps’ and hamstrings’ side-to-side asymmetry in strength would be consistently significant in all stages of chronicity.
As in the previous study, significant weakness was evident in both muscles in all patient groups, ranging from 21% to 32%. Considering the side-to-side asymmetry of ACL deficient knees, the quadriceps deficit persisted through time, whereas the hamstrings regained symmetry even after 1 year without organized rehabilitation. Regarding the side-to-side strength differences, they tended to lower with time, but in the case of quadriceps, they varied from 10% to 23%, whereas the hamstrings were significantly asymmetric only in the short-term group (14%) and acquired acceptable symmetry within 1 year postinjury (Fig. 7-2).
The quadriceps muscle is affected to a greater degree after ACL injury possibly because of (1) postinjury neural inhibition due to the loss of afferent feedback from ACL to gamma motor neurons37,38 and (2) the adaptation toward a “quadriceps avoidance gait” pattern39,40 to prevent anterior subluxation,41,42 which unloads the limb, promoting quadriceps weakness in ACL deficient patients.12 The greater atrophy of the quadriceps (10% versus 4%) reported even 1 year postinjury7 may also add to the explanation of their higher deficit compared with the hamstrings. In contrast, evidence exists that the hamstrings are recruited in weight-bearing activities in a subconscious attempt to counteract anterior shear forces.5,43 This stimulus might have assisted with the improvements in our patients. Evidence in the literature also supports the development of subtle electrophysiological modifications in ACL deficient patients that retune the hamstrings and preprogram their muscle activation strategies to optimize shear force dissipation during injured knee loading.14–16
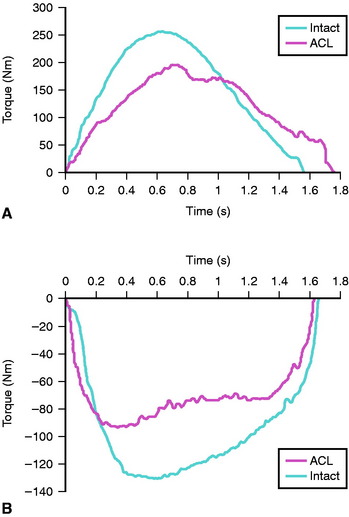
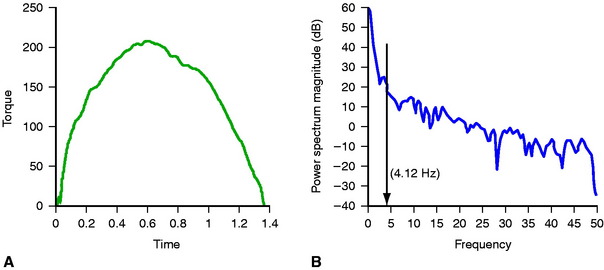
In another study, we investigated the quality of muscle contraction when ACL deficient patients performed maximal exercise via the smoothness of the torque curve throughout knee extension and flexion.44 Our methodology comprised transformation of each torque-time curve pattern into the frequency domain (power spectrum) via fast Fourier transform in order to quantify the smoothness of the isokinetic curve (Fig. 7-3). Each curve of biological signal that is not a perfect sine is actually the sum of other curves, and therefore it can be analyzed into its fundamental components. Our biological interpretation of this method is based on the notion that disturbed motion is generally connected to poor level of joint functionality. Irregular torque output has been connected to other pathologies such as anterior knee pain.45,46 In contrast, smoothness of torque generation is indicative of enhanced force control.47 The frequency contained at three levels of the total power of the signal (90%, 95%, and 99%) was calculated in order to exclude noise from the 100% power level but still include enough harmonics. Both extension and flexion isokinetic curves demonstrated increased irregularities as expressed by the higher-frequency contents by 18.8%, 10.6%, and 40.0% for knee extension and 49.5%, 24.5%, and 16.3% for knee flexion, according to the power level of assessment (Fig. 7-4). Although the results regarding quadriceps were expected on the basis of previous reports using different methodologies, the hamstrings’ increased irregularity had not been reported elsewhere. This finding might be of functional importance and open a future area of investigation.
The higher oscillations characterizing the isokinetic curve of the ACL deficient knee, which is expressed in increased frequency contents, may be attributed to mechanical and/or neuromuscular factors. Increased anterior gliding of the tibia during knee extension might account for the mechanical part. Quadriceps inhibition37,38 and poorly coordinated activation within the hamstrings43,48 must explain the neural aspects of abnormalities of mechanical output. This loss of smoothness in extension-flexion might be clinically important and should be investigated further. Quantification of irregularity of the extension-flexion curve is an innovative approach and could be a valuable tool in the assessment of ACL deficient knees.
Review of the Literature on the Role of the Quadriceps and Hamstrings in Anterior cruciate ligament Deficient Knees
The quadriceps is the muscle group suffering the most dramatic effects after ACL tear.19,30,36,49 For this reason, in addition to its functional importance for normal gait, it attracts most of the attention from clinicians and researchers. Quadriceps torque deficit is more than double hamstring deficit, which is attributed to its susceptibility for quick atrophy due to disuse10,18 and neural inhibition.37,38 Marked weakness of the quadriceps prevents the knee from functioning normally, and given that this weakness is exaggerated in many cases,30 it should be managed adequately. If the voluntary deficit measured via superimposed electrical burst to the maximal voluntary contraction exceeds 5%, treatment with electrical stimulation effectively ameliorates loss of the quadriceps strength and should be implemented from the early stages.50 Although in ACL deficient knees there is no graft to be stressed due to the anterior instability of the tibia caused by quadriceps contraction particularly near extension,9,42,51 this might be harmful for other capsuloligamentous structures.
In contrast, the hamstrings are properly located to counteract anterior tibial instability at flexion angles exceeding 30 degrees.52–54 However, doubts exist regarding the efficacy of the hamstrings to counterbalance shear loading of the knee,53,55 based on two concerns: first, whether the magnitude of the posteriorly directed muscle force is enough to counteract shear forces in the functionally more important knee angles near extension,41,54,56 and second, whether reflex activation of the hamstrings during abrupt perturbations of the knee is fast enough to develop tension in time with the peak external destabilizing moment.57,58
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


