CHAPTER 23 Non-endoscopic limited incision browlift
History
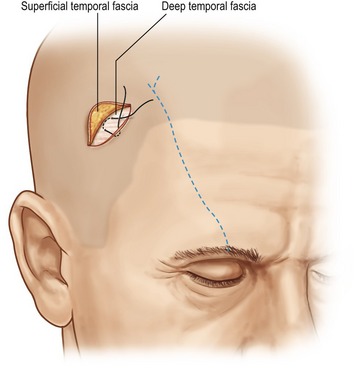
Unfortunately, all these methods have their deficiencies. In particular, the coronal browlift is plagued with a long incision which is feared by patients. Chronic dysesthesia and some scar alopecia are common. Cutaneous approaches leave scars which can be acceptable, but often are not. Browpexy procedures have proven to be inconsistent especially in the presence of mobile skin. Similarly, Knize’s procedure seems successful in some cases but not in others – presumably because of a fixation vector which is directed fairly laterally (Fig. 23.1).
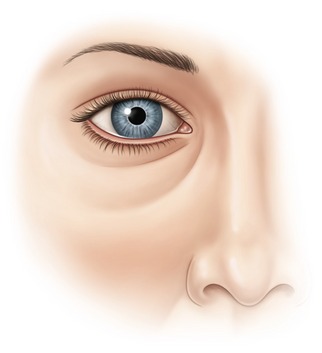
From a surgical perspective, endoscopic brow lifting is an attractive option. It promises minimal incisions, minimal sensory change and little or no hair loss. Numerous authors have demonstrated the success of endoscopic brow surgery by measuring the amount of eyebrow elevation achieved from fixed orbital points. While clearly effective between the medial canthus and the lateral canthus, results at the lateral tail of the eyebrow can be unreliable. The example in Figs 23.2–23.4 illustrates the problem.



Physical evaluation
• Orbit: the size and shape of the orbit, the level of supra-orbital rim, and the relative prominence of the globe within the orbit.
• Hair: the thickness and color of hair and the level of the hairline.
• Forehead skin: the number and depth of the transverse forehead furrows and the depth of the frown lines.
• Eyebrows: the density and color of the eyebrow hairs, the level of the eyebrows in relation to the supraorbital rim and the upper lid sulcus, the relative height of the medial brow to the lateral brow, and the shape of the eyebrow arch.
• Upper eyelids: the level of the lids (normal, ptotic or retracted), the amount of soft tissue fullness above the upper lid sulcus, and the amount of visible eyelid between the eyelashes and the sulcus.
• Muscles: the strength and resting tone in the frontalis, the orbicularis oculi, and the frown muscle complex: the corrugator supercilii, the depressor supercilii, and the procerus.
• Symmetry: of orbital size shape and position, of eyebrow level, and of eyelid level.
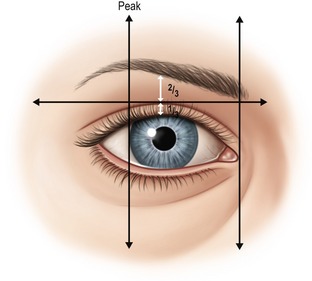
Many different professionals, including cosmetologists, anatomists and plastic surgeons have attempted to define the ideal position and shape of the eyebrow complex. This was reviewed by Gunter who concluded that the aesthetic ideal must be considered in relation to gender, ethnicity, orbital shape, eye prominence and facial proportions. Conventional descriptions of the “ideal eyebrow” in the modern era typically include the following (Fig. 23.5):
1. The medial eyebrow should be at or below the level of the orbital rim.
2. The medial border of the eyebrow should be above the medial canthus.
3. The eyebrow should rise gently, with a gentle peak at least two thirds of the way to its lateral end, and with this peak usually above the lateral limbus.
4. The lateral tail of the brow should be higher than the medial end.
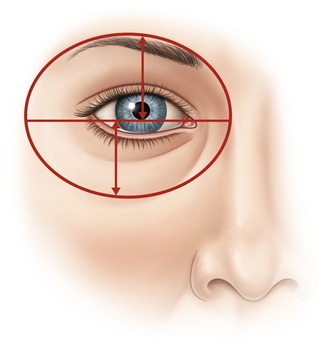
Gunter also observed that the eyebrow and the nasojugular fold create an oval with the pupil at the center of the oval. If the distance from center of the pupil to the eyebrow is reduced, the brow looks low (Fig. 23.6).
The amount of visible eyelid from the lash line to the palpebral fold should be approximately one-third the distance from the lash line to the eyebrow, and not more than one-half (Fig. 23.7).