Introduction
The pathogenesis of hidradenitis suppurativa (HS) remains to be fully elucidated. Genetic susceptibility along with hormonal fluctuations and immune dysregulation are all thought to contribute to HS development. HS tends to occur in patients with comorbid conditions associated with hyperandrogenism, insulin resistance, and inflammation including acne vulgaris, hirsutism, diabetes, and polycystic ovary syndrome (PCOS). Utilizing multimodal treatment regimens including hormonal therapies (anti-androgens, anti-diabetics), systemic immunomodulators (oral retinoids), and immunosuppressants may alleviate HS symptoms and aid in recovery. This chapter discusses non-antibiotic and non-biologic systemic therapies for HS. Table 17.1 summarizes the mechanism of action, other indications, dosing regimen, contraindications, and adverse effects for the medications discussed in this chapter. Table 17.2 outlines the levels of evidence and recommendations regarding the use of these therapies according to the 2019 North American guidelines.
| Medication | Mechanism of Action | Other HS-related Indications | Dosing Regimen | Absolute Contraindications | Relative Contraindications | Adverse Effects |
|---|---|---|---|---|---|---|
| Combined Oral Contraceptives |
|
| Estrogen content < 50 mcg/day PO. Avoid progestogen-only regimens. |
|
|
|
| Spironolactone |
|
| 25–50 mg/day titrate as needed to a dose of 50–200 mg/day, PO |
|
|
|
| Finasteride |
|
| 2.5–10 mg/day PO |
|
|
|
| Metformin |
|
| 1500–2000 mg PO |
|
|
|
| Liraglutide |
|
| 0.6–1.8 mg injection/day |
|
|
|
| Oral Retinoids: Acitretin/Isotretinoin |
|
| 0.5–0.6 mg/kg/day PO |
|
|
|
| Colchicine |
|
| 0.5 mg PO BID |
|
|
|
| Methotrexate |
|
| Start: 15 mg/week with laboratory monitoring Dose adjustments: increase by 5 mg/week at week 8 if no response |
|
|
|
| Dapsone |
|
| Start at 25 mg daily and titrate to 100 mg PO BID |
|
|
|
| Prednisone |
|
| 10 mg/day PO |
|
|
|
| Cyclosporine 42–44 |
|
| 1–6 mg/kg/day |
|
|
|
| Therapy Name | Evidence Level | Recommended Use |
|---|---|---|
| OCPs | A | Consider in female patients with no contraindications. |
| Spironolactone | C | Consider in female patients with no contraindications. |
| Finasteride | D | Not enough evidence to make a definitive conclusion. |
| Metformin | C | Strongly consider in patients with obesity, insulin resistance and/or PCOS. |
| Liraglutide | E | Not enough evidence to make a definitive conclusion. |
| Isotretinoin | C | Not enough evidence to make a definitive conclusion. Consider in patients with severe concomitant acne. |
| Acitretin | B | Consider in patients with recalcitrant HS with failure to respond to first-line therapy. |
| Colchicine | B | Consider in patients with refractory mild-moderate disease who can tolerate colchicine and minocycline combination therapy. |
| Methotrexate | C | Not enough evidence to make a definitive conclusion. |
| Dapsone | B | May be effective for select patients without contraindications. |
| Prednisone | C | Can be used as rescue therapy or bridge-therapy to other long-term treatment option. |
| Cyclosporine | E | Consider in patients with recalcitrant moderate to severe HS who have failed or are not candidates for standard therapy. |
Hyperandrogenism and Hidradenitis Suppurativa
Small questionnaire-based studies conducted in the U.K. found that approximately 50% of women with HS report acute flares which are temporally related to menstruation. In one cross-sectional study in the Netherlands, patients reported frequent changes in disease activity during pregnancy. Furthermore, improvement in HS symptoms during pregnancy was associated with a history of premenstrual disease flares. These findings suggest that disease activity in women with HS may be strongly correlated with hormonal fluctuations.
The skin has the unique ability to synthesize androgens de novo from cholesterol in the epidermis and sebaceous glands. However, the main source of androgens are the testes, ovaries, and adrenal glands. The circulating androgens, dehydroepiandrosterone (DHEA) and androstenedione, are converted into testosterone in sebocytes, sweat glands, and dermal papilla cells. In the skin, the enzyme 5α-reductase metabolizes testosterone into a more potent androgen, dihydrotestosterone (DHT). In comparison to testosterone, DHT binds to androgen receptors with 10 times higher affinity and with greater stability. Androgen metabolism is depicted in Fig. 17.1 .
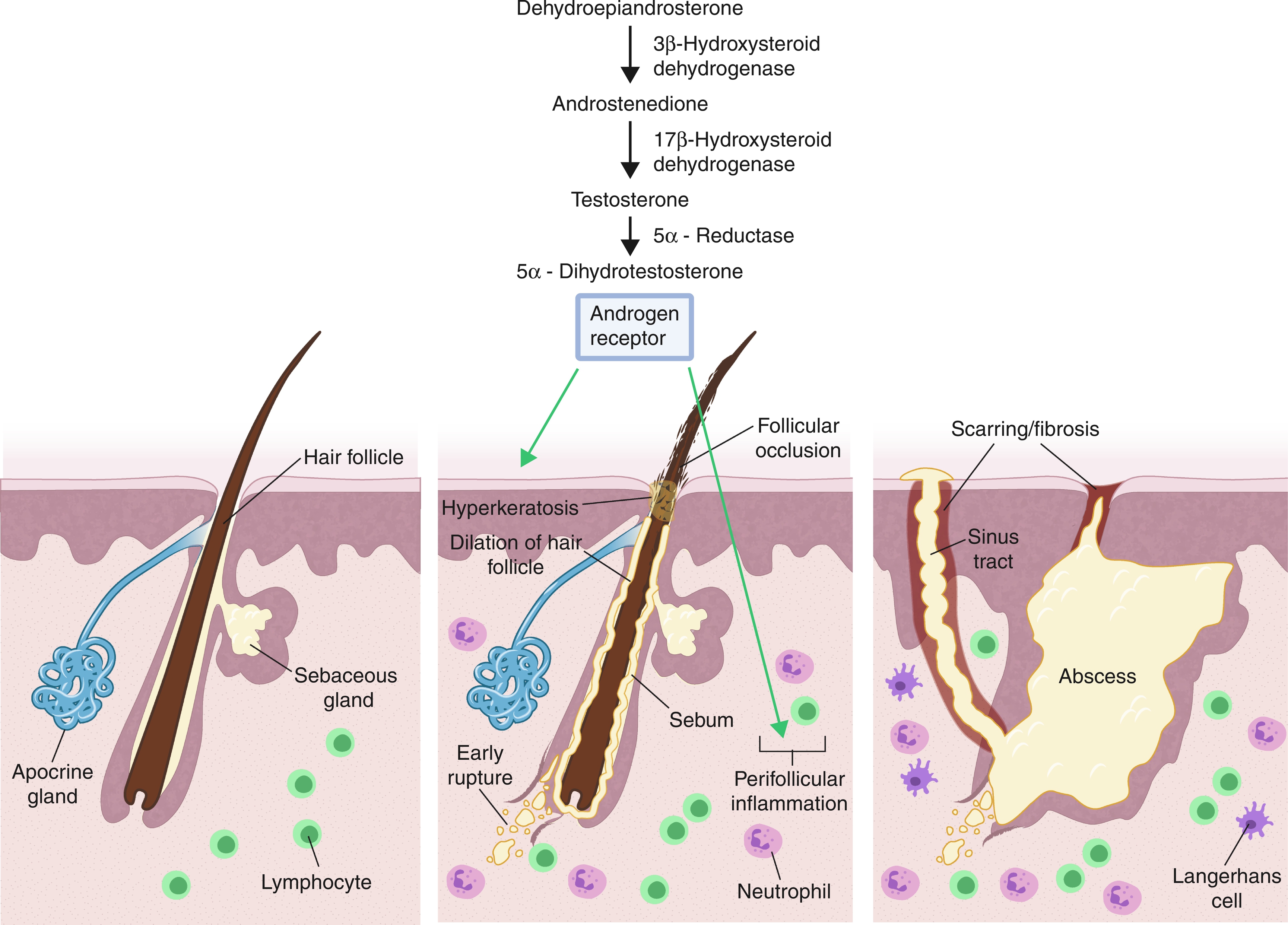
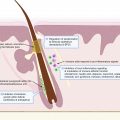
In the skin, androgen receptors are primarily located in the dermal papillae, sebaceous epithelium, eccrine sweat epithelium, and, to a lesser degree, in basal epidermal cells and reticular dermal fibroblasts. They are also present in pilosebaceous duct keratinocytes and, to a lesser degree, in interfollicular keratinocytes, and could play a role in acne and HS via promotion of follicular hyperkeratinization. According to the acne model, hyperproliferation of the infrainfundibular keratinocytes is one of the initial and most crucial events in the development of microcomedones, and is also characteristic of HS. Infrainfundibular hyperkeratosis, hyperplasia of the follicular epithelium, and perifolliculitis lead to localized inflammation and precede follicular rupture in HS. In one study, anti-androgens were shown to decrease follicular debris at the hair follicle, raising the possibility that androgens could play a role in hyperkeratinization. Additionally, increased 5α-reductase activity in infrainfundibular keratinocytes—as opposed to interfollicular epidermal cells—suggests that DHT could affect follicular keratinization; however, this remains to be fully explored.
Androgens may also modulate the inflammatory milieu important in HS pathogenesis. It is postulated that Tumor Necrosis Factor alpha (TNF-α expression, interleukin (IL)-1β, and IL-17 are prominent inflammatory actors in HS. Multiple independent studies have indicated increased IL-17 expression in HS lesions compared with control skin. IL-17 is produced by T-helper-17 (Th17) cells, innate lymphoid cells, T cells, mast cells, and neutrophils. IL-1β, IL-6, TGF-β, and IL-2, produced by innate immune cells, can further upregulate IL-17 production. Testosterone and DHT modulate TGF-β, IL-6, and TNF-α production, indicating that there is a potential for these androgens to exacerbate HS lesions via the Th17 inflammatory pathway. In a rat model, androgens were shown to exacerbate inflammatory responses resulting in delayed skin healing. Androgens specifically promote inflammation by enhancing local TNF-α expression of TLR stimulated macrophages, thereby inducing the release of proinflammatory cytokines. Androgen receptor signaling also upregulates TNF-α expression via other avenues, including increasing the inflammatory monocyte population via upregulation of CCR2, thereby enhancing monocyte chemotaxis. Gilliver et al. conducted a study in which a 5α-reductase inhibitor administrated to a rat model resulted in significantly decreased inflammatory markers such as TNF-α and IL-6 in the skin and markedly accelerated wound healing.
Studies have demonstrated improvement in HS disease activity with the use of both antiandrogens (e.g., finasteride, flutamide, spironolactone) and oral contraceptive pills (OCPs). While the exact mechanism remains unclear, clinical evidence suggests that blocking the androgenic pathway is effective in management and will be discussed below in further detail.
Oral Contraceptives
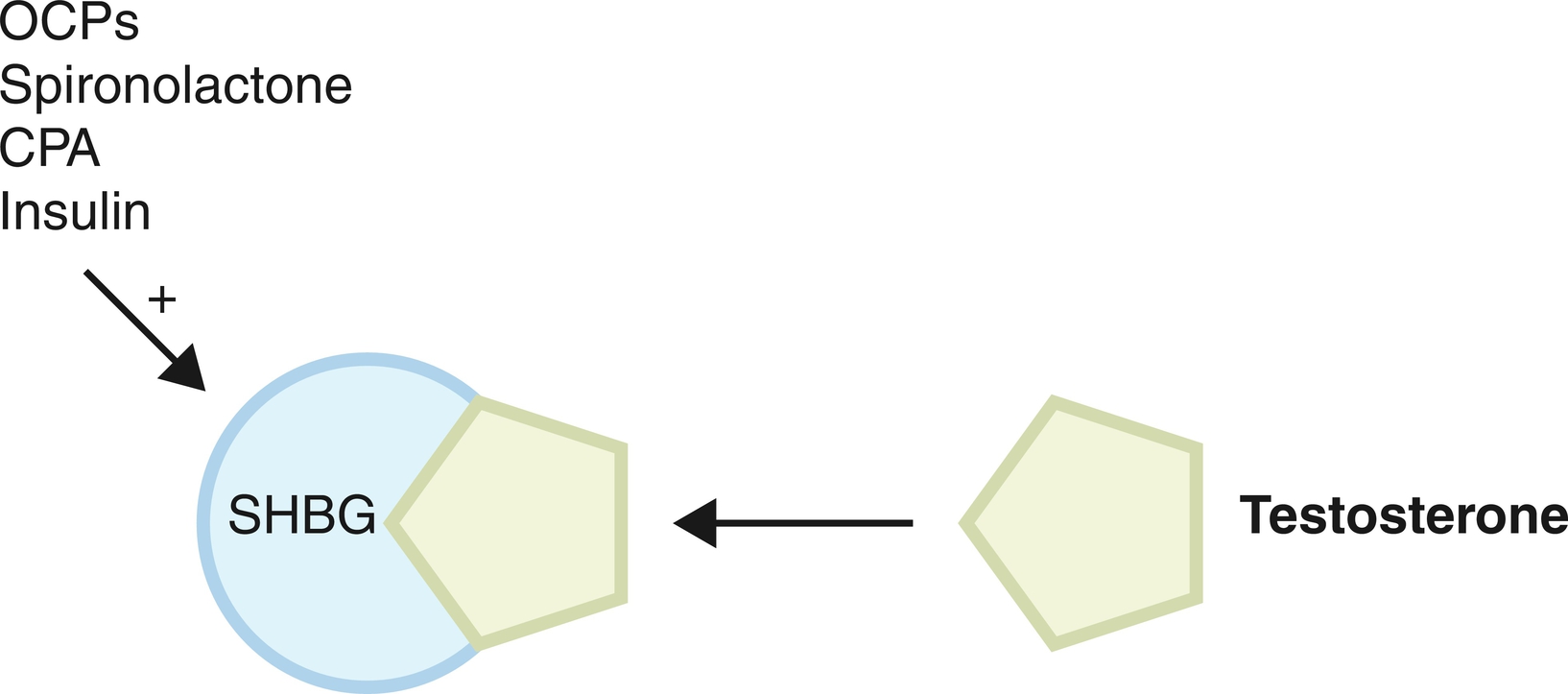
Combined OCPs contain both progesterone and estrogen and act primarily by preventing ovulation through the inhibition of follicular stimulating hormone (FSH) and luteinizing hormone (LH). Oral estrogens produce an anti-androgenic effect by increasing the concentration of circulating sex hormone binding globulin (SHBG). SHBG binds more avidly to androgens than estrogens, rendering androgens less bioavailable to interact with the androgen receptor as demonstrated in Fig. 17.2 .