Key points
Chief complaints for lower eyelid blepharoplasty
- •
Puffiness
- •
Dark circles
- •
Discolored skin
- •
Excess skin
- •
Loose skin
- •
Wrinkled skin
- •
Crows feet
- •
Baggy lids
- •
Sad look
- •
Tired look
- •
Drooping
Lower blepharoplasty is one of the most common cosmetic procedures performed. It requires a thorough understanding of eyelid anatomy and function. The surgeon develops lower blepharoplasty techniques based on knowledge, experience and comfort level that will produce aesthetically pleasing results with the least amount of patient dissatisfaction. Complications that result from lower blepharoplasty are in the range of 1–2%. The most problematic complication is lower eyelid malposition caused by orbicularis oculi muscle impairment with potential corneal exposure and ocular injury.
We have developed a lower blepharoplasty technique that produces an aesthetic result with the least potential of creating a lower eyelid malposition due to orbicularis oculi muscle impairment. The no touch lower blepharoplasty is performed with or without concomitant upper blepharoplasty.
The principle tenet of the technique is to not touch the pretarsal orbicularis oculi muscle, therefore, minimizing the potential for muscle impairment. This is accomplished by approaching the lower eyelid anatomy with a transconjunctival, retroseptal access. The completion of the lower blepharoplasty includes arcus marginalis release with lower eyelid fat transposition, lateral upper eyelid access incision for lower eyelid lateral fat modification, inferior retinacular lateral canthopexy or canthoplasty for orbicularis oculi tightening and redraping, and excision of excess lower eyelid skin by a pinch technique.
We have found the no touch lower blepharoplasty technique to be anatomically sound and easy to learn, perform and teach. Eyelid malposition due to pretarsal orbicularis oculi muscle impairment can be avoided with this technique.
The no touch lower blepharoplasty incorporates procedures that solve the anatomical problems of excess skin, fat protrusion, horizontal lid laxity and lateral canthal shift.
In general, the lower blepharoplasty requires knowledge of how to manipulate anatomy by mastering technical skills.
The various surgical techniques and their sequence are based on the chief complaint, the medical and ophthalmological history, and the physical examination. Another major factor is the surgeon’s experience, preference and comfort level in performing lower blepharoplasty. The lower eyelid anatomy can be approached via transcutaneous, skin–muscle flap or transconjunctival access. A patient with prominent globes and malar hypoplasia who also has lower eyelids with fat protrusion, scleral show and significant horizontal eyelid laxity requires a comprehensive lower blepharoplasty. The techniques chosen should provide safe, reproducible and specific solutions to modify the lower eyelid anatomy to a favorable aesthetic and functional result. It may require modified reconstructive procedures such as transconjunctival retroseptal orbital exploration, lateral canthoplasty, horizontal lid tightening and orbicularis oculi muscle redraping.
This type of intervention is better termed a comprehensive blepharoplasty because it requires knowledge of reconstructive and aesthetic techniques. Each surgeon develops his own comprehensive blepharoplasty that satisfies his preference, comfort level, experience and outcome standards.
We recommend a blepharoplasty technique which has been developed over the past 25 years with an experience of over 5000 lower blepharoplasties. The technique is termed the ‘no touch’ lower blepharoplasty because it performs the operation without damage to the pretarsal orbicularis oculi muscle. It also limits the surgical manipulation of the mid lamella of the lower eyelid (see Fig. 6.6 ), thus lessening the chance of cicatrical vertical contracture. When a comprehensive lower eyelid blepharoplasty is required we prefer the no touch technique. When the clinical situation in the lower eyelid is less complicated this technique is also preferred because it produces predictable, aesthetic results.
History
The transconjunctival lower blepharoplasty was described by to address those patients with primarily fat protrusion with little or no skin excess. advanced the use of the transconjunctival approach in older patients. The skin-muscle flap of McIndoe popularized by , and Aston (1982) was widely used for management of excess fat protrusion and skin of the lower eyelids. Castanares (1951) and Klatsky & Manson (1981) described a skin approach to lower blepharoplasy which allowed differential removal of excess skin and muscle.
Lateral canthorrhaphies were developed to avoid the deformaties associated with tarsorrhaphies. These procedures were various flap transpositions with skin removal to support the lower eyelid to the upper eyelid at the lateral canthus. Denonvilliers (1856, 1863), Kuhnt-Szymanowski (1870, 1912, 1916) and Meller (1953) described procedures that were widely accepted. Modifications of these procedures were described by Smith (1959) and Kazanjian & Converse (1959) with a tarsoconjunctival wedge excised medially. Bick (1966) reported a technique removing the full-thickness temporal aspect of the lower eyelid to correct laxity. Edgerton & Wolfert (1969) described a de-epithelialized dermal pennant of lateral canthal tissue that was passed through a drill hole in the lateral orbital wall to correct lower eyelid malposition. Montandon (1978) modified this procedure to include a lateral tarsorrhaphy. Lateral canthal suspensions have also been described by Whitaker (1984) via the face lift; Whitaker (1984), Ortiz-Monastario & Rodriguez (1985) from the coronal, and Paterson et al (1987) from the conjunctival approach. Jelks (1990, 1991, 1993, 1995), Hinderer (1993), and Carraway (2001) described variations in bony fixation of the lower eyelid.
Many surgeons developed their own methods of creating the lateral canthal angle by various lateral canthal tendon suture techniques. The most effective methods isolated the lower lid contribution to the lateral retinaculum by a lateral canthotomy and cantholysis of the inferior limb of the lateral canthus at the bony orbital rim. The lower eyelid was thus released from the upper eyelid and retinacular structures to allow more selective repositioning. Tenzel (1969), Marsh & Edgerton (1979), Bachelor & Jobe (1980), Holt et al (1984) and Leone (1987) described the use of periosteal flaps and temporalis fascia and palmaris longus tendons for lateral canthal reconstructions.
Anderson & Gordy (1979), Hamako & Baylis (1980), Wesley & Collins (1983), Lisman et al (1987), , Patipa (1999), Fagien (2002), McCord (2002), Hester (2004) and Codner (2006) have described various methods of tarsal and/or inferior retinacular attachment to the bony orbital tissues that selectively tighten and reposition the lower eyelid.
Anatomy
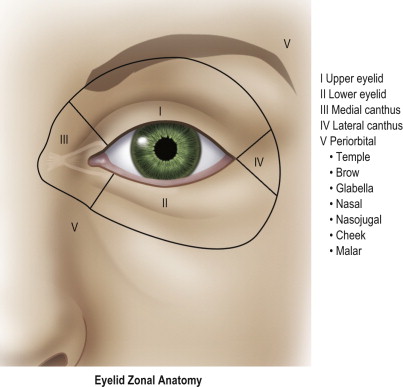
To facilitate a thorough anatomical analysis, the eyelids and surrounding structures are divided into zones ( Figures 6.1, 6.2 ).
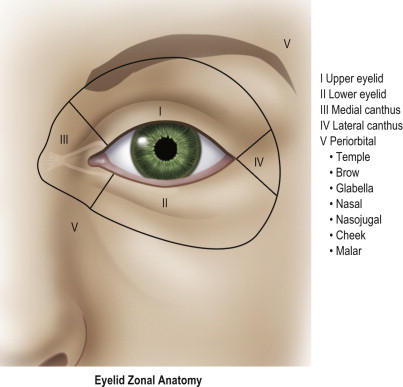
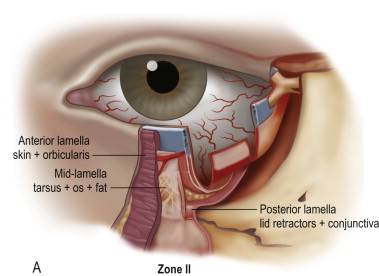
The lower eyelid (zone II) extends from the lid margin to the inferior orbital bony rim. It is separated into the anterior lamella of skin and orbicularis oculi muscle, the middle lamella consisting of tarsus, orbital septum and retroseptal fat and the posterior lamella with the capsulopalpebral fascia or lower eyelid retractors and the conjunctiva ( Figure 6.2A ).
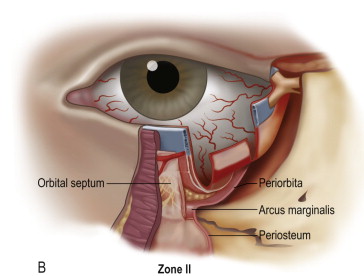
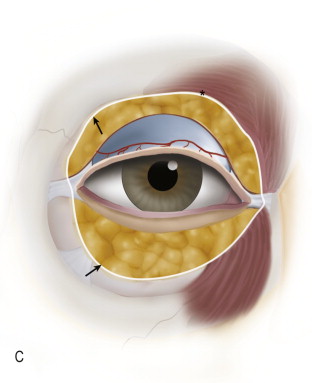
The confluence of the orbital septum, orbital floor periorbita and maxillary periosteum at the inferior bony margin is termed the arcus marginalis ( Figure 6.2B ). The arcus marginalis in the inferior medial orbit corresponds to the origin of the orbital portion of the orbicularis oculi muscle ( Figure 6.2C ).
The orbicularis oculi muscle is innervated by the seventh cranial nerve and acts as an antagonist to the levator palpebrae superioris muscle innervated by the third cranial nerve. The orbicularis oculi muscle is divided into palpebral and orbital portions. The palpebral portion is further subdivided into pretarsal and preseptal portions. The orbital portion of the orbicularis oculi arises medially from the superiormedial orbital margin, the maxillary process of the frontal bone, the medial canthal tendon, the frontal process of the maxilla, and the inferiormedial orbital margin ( Figure 6.2C ).
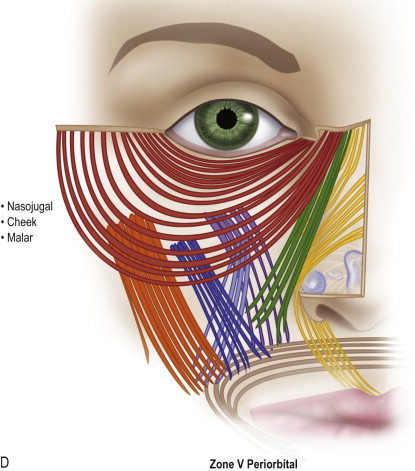
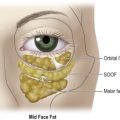
The peripheral fibers sweep across the eyelid over the orbital margin in a series of concentric loops, the more central ones forming almost complete rings. In the lower eyelid, the orbital portion covers the origins of the elevator muscles of the upper lip and nasal ala and continues temporally to cover part of the origin of the masseter muscle. Occasionally, the lower orbital portion may actually continue as low as the corner of the mouth. The inferior orbital orbicularis oculi constitutes the nasojugal, cheek and malar area of the facial anatomy ( Figure 6.2D ).
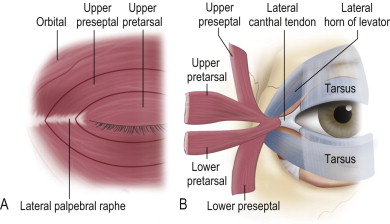
The preseptal portion diverges from its origin on the medial canthal tendon and posterior lacrimal diaphragm and passes across the lid as a series of half ellipses to meet at the lateral palpebral raphe ( Figure 6.3A ). The muscle bundles are not interrupted and do not interdigitate at the raphe. The pretarsal muscles form a more superficial common lateral canthal tendon 7 mm from the lateral orbital tubercle where it inserts ( Figure 6.3B ).
The medial canthus (zone III) is a complex region containing the origins of the orbicularis oculi muscle and the lacrimal collecting system ( Figure 6.4 ).
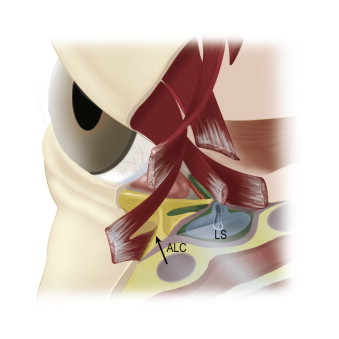
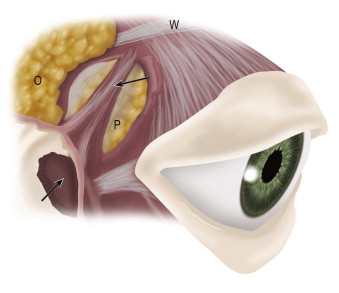
The lateral canthus (zone IV) is an integral anatomic unit of the temporal aspects of the eyelids. The lateral canthus is more correctly termed a lateral retinaculum which consists of the lateral horn of the levator palpebrae superioris muscle, the continuation of the preseptal and pretarsal orbicularis oculi muscle as the lateral canthal tendon, the inferior suspensory ligament of the globe (Lockwood’s ligament) and the check ligaments of the lateral rectus muscle ( Figure 6.5 ). The lateral retinaculum structural components attach to a confluent region of the lateral orbital rim known as Whitnall’s tubercle. It is important to note that the lower eyelid lateral fat is immediately inferior to the lower eyelid contribution to the lateral canthal tendon as it inserts into the orbital tubercle confluence of the lateral retinacular structures. This portion of the lateral canthal mechanism is termed the inferior retinacular component and is the anatomical basis for the inferior retinacular lateral canthoplasty.
Anatomy
To facilitate a thorough anatomical analysis, the eyelids and surrounding structures are divided into zones ( Figures 6.1, 6.2 ).
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


