Key Words
nipple-sparing mastectomy, breast cancer, breast reconstruction, nipple–areola complex
Introduction
Nipple-sparing mastectomy (NSM) is the most recent advancement in the surgical management of breast cancer, allowing for complete preservation of the nipple–areola complex along with the breast skin envelope. Initially, NSM was largely limited to utilization in prophylactic cases. As experience with this technique has grown, oncologic safety has been demonstrated as comparable to skin-sparing and total mastectomy. As such, indications for NSM have expanded to therapeutic cases, including those with more advanced breast disease. Options for breast reconstruction after NSM include the full range of alloplastic and autologous techniques. Importantly, NSM has been shown to significantly improve post-reconstruction patient-reported satisfaction and quality of life compared to non-NSM techniques.
Reconstructive outcomes with NSM continue to be defined. Numerous patient-, operative-, and technique-specific factors have been demonstrated to variably influence outcomes. Overall, reconstructive safety has been demonstrated in implant-based and autologous breast reconstruction after NSM with rates of complications generally less than 7%. Nipple-sparing mastectomy does place greater stress on the overlying skin envelope and requires careful preoperative planning as well as meticulous intraoperative technique to ensure successful breast reconstruction.
Indications and Contraindications
Appropriately selecting candidates is perhaps that most important component of successful breast reconstruction after NSM. Primarily, oncologic considerations prevail. While traditional oncologic contraindications for nipple-sparing mastectomy included large tumors and tumors within 1–2 cm of the nipple–areola complex, recent studies have demonstrated oncologic safety in patients with tumors within 1 cm of the nipple–areola complex. Nipple–areola complex tumor involvement has been proposed as the most important oncologic consideration in patient selection for nipple-sparing mastectomy and remains the only absolute oncologic contraindication at our institution. Therefore, all patients undergoing mastectomy for prophylactic indications or for therapeutic indications without clinical nipple–areola complex disease involvement are offered NSM, so long as concurrent reconstructive considerations are met.
Multiple patient and operative risk factors have been variably identified in the literature as increasing risk of reconstructive complications. These include older age, elevated body mass index and mastectomy weight, preoperative radiation and chemotherapy, various mastectomy incisions, and smoking, among others. Data remains conflicting regarding the hazard posed by each individual risk factor. While no single such factor represents an absolute contraindication to NSM, candidates possessing multiple risk factors should be approached cautiously, counseled regarding their increased potential for complications, and may preferentially be offered skin-sparing or total mastectomy.
In our practice, patients with nipple to sternal notch distances of greater than 25 cm and/or severe grade II or grade III breast ptosis are at higher risk of reconstructive complications and poor aesthetic outcome, representing relative contraindications for NSM. However, patients with macromastia or breast ptosis may undergo NSM in a delayed fashion after staged reduction mammaplasty to reduce the breast envelope and optimize nipple–areola complex position. This is more appropriate in prophylactic cases such that sufficient time, typically three months, may elapse between the reduction mammaplasty and NSM. Lastly, patients with severe chest wall asymmetry or nipple–areola complex asymmetry are at higher risk of postoperative asymmetry and may be best served with skin-sparing techniques. Therefore, the optimal patients for NSM are women with small to moderate-sized breasts with minimal ptosis undergoing mastectomy for prophylactic or therapeutic indications without evidence of nipple–areola complex tumor involvement ( Table 22.1 ).
| Indications | Absolute Contraindications |
|---|---|
| Small-breasted patients Minimal ptosis (grade I to mild grade II) Nipple to sternal notch distance <25 cm | Clinical nipple–areola complex tumor involvement |
| Relative Indications | Relative Contraindications |
| Prophylactic mastectomy indication | Oncologic Large tumors Tumor-to-nipple distance <1 cm Reconstructive Macromastia Nipple to sternal notch distance >25 cm Breast ptosis (severe grade II to grade III) Older patient age Elevated body mass index Higher mastectomy weight Prior chemoradiation Active smoking status Severe chest wall, breast footprint, or nipple–areola complex asymmetry |
Once a patient is established as a candidate for NSM, options for reconstruction must be determined, all of which are available after NSM. Within implant-based reconstruction methods, tissue-expander reconstruction is preferred for those desiring a larger postoperative breast size or patients with asymmetric nipple–areola complexes. Immediate, direct-to-implant reconstruction is reserved for patients with good preoperative nipple–areola complex position who desire a similar postoperative breast size. Placement of immediate, permanent implants greater than 400 mL in volume has been shown to increase the risk of complications in NSM. Therefore, patients in whom predicted permanent implant size is greater than this threshold are best served with tissue expander–based reconstructions. The full range of autologous reconstruction options are also available after NSM.
Preoperative Evaluation
Women presenting in consultation for NSM with immediate breast reconstruction should undergo a comprehensive assessment to determine their candidacy, primarily involving a complete breast examination. Further, a complete history must be ascertained including a determination of past medical and surgical history, body mass index, and smoking status, among other considerations. Specifically related to smoking status, pack-year and time-to-quitting smoking should be determined as patients undergoing NSM with a less than 10 pack-year history and greater than five years-to-quitting smoking have demonstrated equivalent outcomes to non-smokers.
First, bilateral breasts are examined for any obvious or palpable lesions. While palpable or large tumors are not necessarily contraindications for NSM, their presence and location should be noted as they may influence incision choice and/or indicate the potential need for neoadjuvant or adjuvant chemoradiation. Next, the nipple–areola complexes are evaluated for any sign of clinical tumor involvement including palpable subareolar tumors, nipple discharge, and/or peau d’orange. Any evidence of such involvement would represent an absolute contraindication for NSM due to risk of postoperative locoregional disease recurrence of nipple–areola complex origin. Any significant findings related to breast pathology should be discussed with and confirmed by the patient’s surgical oncologist, as both parties must agree that the patient is an oncologic candidate for NSM prior to proceeding.
Once the patient is established as a candidate for NSM from an oncologic standpoint, reconstructive considerations must be evaluated. The overall chest wall and breast footprint(s) are generally examined. While mild to moderate nipple asymmetry may be remedied intraoperatively or in secondary revisions in NSM, severe nipple–areola complex asymmetry is difficult to correct and is a relative contraindication to NSM. The breast is also examined for prior surgical scars that may be incorporated into the ultimate incision utilized for NSM. Periareolar scars should be carefully examined as more recent incisions may compromise blood supply while older scars may serve as a delay to the nipple–areola complex, improving perfusion.
Breast size and ptosis are next evaluated. Standard breast measurements, including nipple to sternal notch distance, nipple to inframammary fold distance, and base width should be measured. Patients with small to moderate-sized breasts and grade I to mild grade II ptosis (sternal notch to nipple distance less than or equal to 25 cm) represent the best candidates for NSM. Macromastic patients or those with severe grade II to grade III ptosis (sternal notch to nipple distance greater than 25 cm) should be approached cautiously. These patients are at greater risk of poor perfusion, ischemic complications, postoperative nipple malposition, and poor aesthetic result. Therefore, patients with larger or more ptotic breasts are best served with skin-sparing techniques or undergoing delayed NSM after staged reduction mammaplasty. Immediate breast reconstruction in NSM using a skin reduction pattern incision is possible but is prone to high rates of wound healing complications.
The quality and laxity of the breast envelope is also assessed. Good breast skin quality and minimal laxity, represented by a pinch test of greater than 2 cm and snap-back in each breast quadrant, are optimal for NSM. In these patients, the breast-skin envelope can accommodate well to the underlying reconstruction, whether alloplastic or autologous.
Once a patient has been determined to be a candidate for NSM from both an oncologic and reconstructive perspective, options for reconstruction should be discussed with the patient. While no algorithm exists to predict individualized risk of complications in NSM, a discussion should also take place regarding present risk factors and their potential influence on the perioperative risk profile of each individual patient. Patients must be counseled on the possibility of adjustments to the operative plan based on intraoperative findings that may require removal of the nipple–areola complex or conversion from a one-stage to a two-stage alloplastic reconstruction. Factors requiring such adjustments may include positive findings of subareolar biopsy or evidence of poor perfusion upon assessment of the mastectomy flaps intraoperatively. If the intraoperative nipple biopsy is positive for cancer or the nipple is found to be ischemic and requires excision, a plan on how to handle the contralateral nipple needs to be discussed.
Surgical Techniques
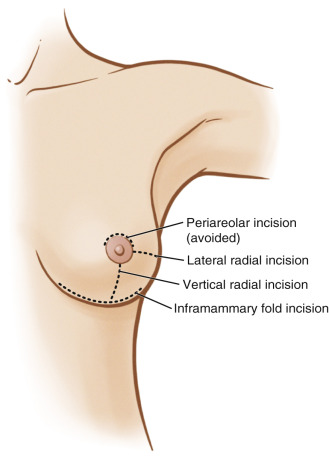
Prior to entering the operating room, the patient’s midline is marked along with the inframammary fold, superior breast border, and planned mastectomy incision. The choice of mastectomy incision is made in concert with the breast surgeon. Lateral radial incisions offer good surgical access for NSM and subsequent reconstruction, making them a good choice for routine NSM in breast cancer patients with implant-based reconstruction. These incisions also can offer access to the axilla for lymph node biopsies. An effort is made in cases of prophylactic NSMs to utilize inframammary fold incisions as they offer the advantage of minimizing the visible postoperative scar burden. Surgical access for mastectomy with inframammary fold incisions is more challenging and is best utilized in patients with small to moderate-sized breasts. Lastly, vertical incisions are utilized preferentially for microsurgical autologous NSM reconstruction as they afford greater access to the internal mammary vessels. Periareolar incisions have been associated with increased complications in NSM and are very infrequently utilized in our practice ( Fig. 22.1 ).
Upon entering the operating room, the patient lies supine on the operating room table with the arms abducted 90 degrees. The breast is infiltrated with a dilute solution of lidocaine and epinephrine. This assists in hydrodissection of the proper mastectomy plane, facilitates a bloodless field, and also improves postoperative pain control and minimizes postoperative nausea and vomiting. One limitation of using this solution is that intraoperative angiography may not be reliably utilized if there is a question of skin flap viability, necessitating reliance on clinical judgment.
Next, NSM proceeds through the chosen mastectomy incision. Great care is taken to perform the mastectomy in the appropriate plane, being at the level of the superficial breast fascia ( ![]() ). This is an anatomic plane that is present, but variably defined, in all individual patients using magnetic resonance imaging ( Fig. 22.2 ). It has been demonstrated that patients with thinner postoperative NSM flap thickness and a reduced post-/preoperative NSM flap thickness ratio have higher rates of reconstructive complications in NSM. This emphasizes the importance of precise dissection at this level to both maximize removal of breast tissue and perfusion of the breast envelope.
). This is an anatomic plane that is present, but variably defined, in all individual patients using magnetic resonance imaging ( Fig. 22.2 ). It has been demonstrated that patients with thinner postoperative NSM flap thickness and a reduced post-/preoperative NSM flap thickness ratio have higher rates of reconstructive complications in NSM. This emphasizes the importance of precise dissection at this level to both maximize removal of breast tissue and perfusion of the breast envelope.
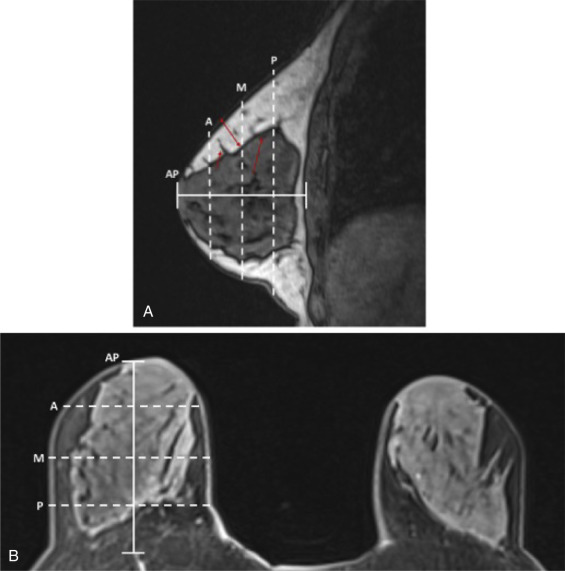
 of AP distance; M, middle measurement at
of AP distance; M, middle measurement at  AP distance; P, posterior measurement and
AP distance; P, posterior measurement and  AP distance; short red arrow, Cooper’s ligament with breast tissue extending to dermis; long red arrow, anterior mammary fascia; double-headed red arrow, example of flap thickness measurement at middle location.
AP distance; short red arrow, Cooper’s ligament with breast tissue extending to dermis; long red arrow, anterior mammary fascia; double-headed red arrow, example of flap thickness measurement at middle location.Related posts:
 Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Fat Grafting as an Adjunct Procedure in Breast Reconstruction
Fat Grafting as an Adjunct Procedure in Breast Reconstruction
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


