Melanocytic nevi (moles) are common benign skin tumors. In most people, these are primarily of cosmetic significance. However, nevi can occasionally become irritated or subjected to trauma and may need to be removed. Most nevi are benign, but, atypical nevi have some features that resemble malignant melanoma, and in certain circumstances the presence of atypical nevi is a marker for an increased risk of developing malignant melanoma.
Melanoma is a potentially deadly cancer whose incidence is on the rise. It is unique among most serious cancers, because it can be detected by both patients and clinicians with a simple skin examination. The clinician can provide a great service to patients by providing a few simple guidelines for the early detection of melanoma.
Melanocytic nevi (moles) are among the most common benign tumors in humans. Nevi are more common in Caucasians. They are less common in Asians and Black individuals. But when they do occur they are more likely to be on the palms and soles. Interestingly, nevi are also less common in patients with the melanocortin-1 receptor (MC1-R) gene pigment variant (red hair, fair skin, always burns).
Nevi appear in early childhood reaching a maximum number in the 3rd to 4th decade of life, with a subsequent decline in number.1 They are more common on sun-exposed skin, as natural sunlight and artificial ultraviolet light are factors in their induction.
Nevi are benign hamartomas of melanocytic nevus cells. They are thought to arise from cells delivered from the neural crest to the skin during embryologic development.
Nevi are usually asymptomatic. Patients may bring nevi to a clinician’s attention because of new onset, growth, symptoms of pain or itch, interference with activities of daily living, or alarming appearance. They may also bring them to attention because of a cosmetically unacceptable appearance.
Nevi are small, circumscribed macules, papules, or nodules. They range in color from blue/black through brown, pink to skin colored. Acquired nevi are almost always less than 1 cm in diameter. Melanocytic lesions greater than 1 cm may be congenital nevi, atypical nevi, or melanoma. Nevi may occur anywhere but there is a predilection to sun-exposed skin.
Common presentations of nevi:
Junctional nevi arise at the skin dermal–epidermal junction; they are typically macular (Figure 18-1).
Intradermal nevi present with nevus cells confined to the dermis of the skin and are papular (Figure 18-2).
Compound nevi have both junctional and dermal components and are usually papular.


Less common presentations of nevi:
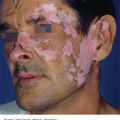
Halo nevus (Sutton nevus): These are usually benign melanocytic nevi surrounded by a halo of depigmentation (Figure 18-3), which may be due to a direct cytotoxic effect of lymphocytes surrounding the nevus. The halo usually heralds involution of the nevus over months to years. These lesions most commonly occur in childhood. Patients may have associated vitiligo. Melanoma can masquerade as a halo nevus, and melanomas in other sites may precipitate halo nevi. The presence of a halo nevus warrants a total skin examination and any atypical feature of the nevus itself justifies removal and histopathological examination.
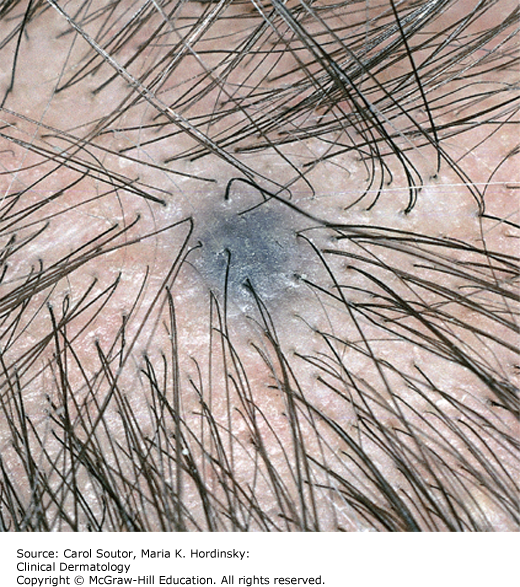
Blue nevus: These are acquired nevi that range in color from blue to black (Figure 18-4). The onset is usually in childhood, with predominance in Asians. These nevi are benign, but melanoma, especially nodular melanoma may masquerade as a blue nevus. Indications for biopsy include atypical features such as size >1 cm or irregular shape or color, late onset, or a changing lesion.
Spitz nevus: These are small, typically pink or tan nevi that appear suddenly, primarily in children. They have characteristic dermoscopic and histopathological features. Spitz nevi are unusual in patients over the age of 40; therefore, skin lesions with the dermoscopic features of Spitz nevi are best removed in this age group to exclude melanoma with Spitzoid features.

Features in a nevus that are signs that may indicate a melanoma are listed in Table 18-1.
The histopathologic findings of common acquired melanocytic nevi show mature melanocytes arranged as individual cells or in nests. The margin of the nevus is discrete.
Common acquired melanocytic nevi present as tan, brown, or black macules or papules or skin-colored papules with uniform colors and borders.
The adoption of dermoscopy has enhanced the ability of the clinician to differentiate normal nevi from atypical nevi and melanomas (Figures 18-5 and 18-6).2 Dermoscopy uses an illuminated, high quality 10×-magnifying lens coupled to a device to remove surface reflection. This is done either using a set of cross-polarizing filters (polarized dermoscopy) or by direct contact with the skin using a coupling liquid such as an alcohol-based hand cleansing gel. The limitation of dermoscopy is that it is learning intense, but there are a number of algorithms that have been designed to assist clinicians in making the decision to biopsy suspicious lesions.


The easiest is the 3-point algorithm that uses 3 simple criteria for the analysis of a melanocytic neoplasm: (1) the presence of an atypical pigment network; (2) asymmetry of any structure; and (3) the presence of any structure that is blue or white. The presence of 2 or more criteria warrants a removal of the lesion for histopathologic examination.2 A full body dermoscopic examination typically takes about 2 to 3 minutes.
✓ Table 18-2 lists the differential diagnosis for common acquired nevi, which primarily includes other pigmented tumors.
Differential diagnosis of pigmented tumors.
| Pigmented Lesion | Clinical Findings |
|---|---|
| Benign nevus | Symmetric, uniform color and border, size usually <6 mm, resembles other nevi on a patient (Figures 18-1 and 18-2) |
| Atypical nevus | Size >6 mm, asymmetric, irregular color or border, appears different than other moles on a patient (Figure 18-7) |
| Congenital nevus | Present at birth. Often greater than 1 cm in size by adulthood (Figure 18-8) |
| Melanoma | Features similar to atypical nevus. Changing or symptomatic lesion (Figures 18-9, 18-10, 18-11, 18-12, 18-13) |
| Lentigo | Evenly colored, sharply marginated, resembles other lentigos in sun-damaged skin (Figure 16-4) |
| Seborrheic keratosis | Warty, with typically a “stuck-on” appearance, sharp round border (Figure 16-1) |
| Pigmented basal cell cancer | May be indistinguishable from melanoma (Figure 17-4) |
| Dermatofibroma | Even color or lighter center, puckers when pinched (Figure 16-5) |
| Becker’s nevus | Large unilateral brown patch on shoulder or chest, may have increased hair |
Nevi are usually asymptomatic. Patients who have more than 50 nevi are at increased risk for developing melanoma and they should have a full body skin examination annually.3 They should be counseled on sun precautions and how to perform self-examination.
If feasible, clinically suspicious nevi should always be removed in their entirety so that the entire lesion can be examined histopathologically. Clinically suspicious lesions often have one or more of the following features of the ABCDE rule (Table 18-1). Melanocytic lesions are also suspicious for melanoma if they are painful or pruritic or if the lesion becomes eroded in the absence of trauma. Dermoscopy aids in the evaluation of nevi and other cutaneous neoplasms.
Consideration for referral for regular screening should be given in patients with multiple nevi, especially if the clinician is uncomfortable with dermoscopy.
Depending on the surgical skills of the clinician, patients may be referred for excision of particularly large nevi or nevi in cosmetically sensitive areas.
American Academy of Dermatology: www.aad.org/skin-conditions/dermatology-a-to-z/nevi
Atypical nevi (dysplastic nevi) may occur sporadically as isolated “ugly ducklings” (nevi that appear different from other nevi on the body) or as multiple lesions as in the case of atypical nevus syndrome. They can appear in adulthood or childhood and are not uncommon, occurring in up to 5% of Caucasians. They are present in virtually every patient with familial cutaneous melanoma and in 30% to 50% of patients with sporadic primary cutaneous melanoma. Risk factors include a history of sun exposure, but atypical nevi can occur in sun-protected skin. Unlike common acquired nevi, new atypical nevi continue to appear throughout a patient’s lifetime.
Atypical nevus syndrome describes an autosomal dominant phenotype of patients with multiple nevi of different sizes and colors. Patients with atypical nevi have an increased risk for melanoma. The general population has a 1.93% life-time risk for melanoma. The following are the approximate life-time risks (%) of melanoma for patients with atypical nevi.
5% for one atypical nevus with increasing risk for additional atypical nevi
18% for atypical nevus syndrome
100% for atypical nevus syndrome with two blood relatives with melanoma
Atypical nevi are often thought of as melanoma precursors, but this concept is controversial. Most authorities consider atypical nevi as potential markers for an increased risk for developing melanoma de novo. The other important significance of atypical nevi is the potential histopathologic ambiguity and the risk of under diagnosis of melanoma.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


