Neoplasms of Subcutaneous Fat: Introduction
|
Lipoma
|
Lipomas are the most common soft-tissue neoplasm. Although they affect individuals in a wide age range, they occur predominantly in adults between the ages of 40 and 60 years; presentation in childhood is rare. There is no gender predilection. Lipomas are multiple in approximately 5% of cases.1
The majority of lipomas (approximately 75%) show karyotypic abnormalities. The cytogenetic findings are heterogeneous, but rearrangements of 12q13–15 are most common.2–4 Other affected loci are on chromosomes 6 and 13.2–4 Numerical abnormalities are scarce, and most tumors are diploid.
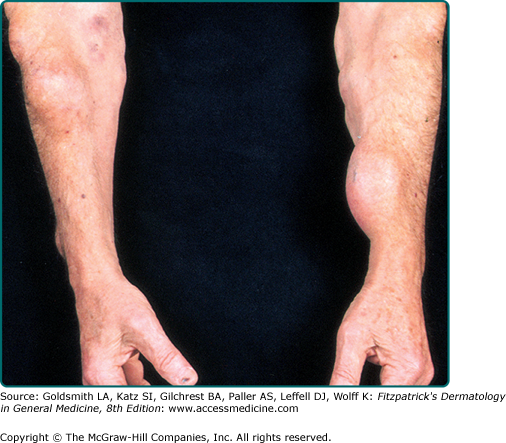
The most common presentation is as a painless, slowly enlarging mass involving the subcutaneous tissue of the trunk, neck, or proximal extremities. Involvement of the head, hands, and feet is uncommon. These superficial lipomas are typically small, measuring less than 5 cm.1 Lipomas may be multiple and familial and show a predilection for the arms and thighs in familial multiple lipomatosis (Fig. 129-1).5 The constellation of multiple lipomas, macrocephaly, lymphangiomas, and hemangiomas is known as Bannayan (Bannayan–Zonana) syndrome.6,7 This autosomal dominant disease shares features with other independently described entities and is currently also referred to as Bannayan–Riley–Ruvalcaba syndrome.8,9 Further clinical findings include intestinal polyposis, genital pigmented macules, and other hamartomas. The syndrome is caused by mutations in the PTEN gene and belongs to the larger family of PTEN hamartoma-tumor syndromes, including Cowden disease.10–15 Lipomas may also be seen as a manifestation of Gardner’s syndrome. Gardner’s syndrome is part of the spectrum of familial adenomatous polyposis and includes extracolonic manifestations such as desmoid fibromatosis, osteomas, cysts, and lipomas.
Less frequently, lipomas may be deep-seated and grow to sizes larger than 5 cm. They can affect a variety of anatomic locations, including the surface of bone (parosteal lipoma) and skeletal muscle (intramuscular and intermuscular lipoma). Intramuscular lipoma arises within skeletal muscle and may be circumscribed or infiltrative. It presents in adulthood and only rarely affects children. The range of anatomic sites is wide, but there appears to be a predilection for the trunk.16,17 In contrast, intermuscular lipoma develops between individual muscles and does not infiltrate skeletal muscle bundles. It is a rare lipomatous tumor with a predilection for the anterior abdominal wall.16,17 Lipomas of the forehead are frequently deep-seated, presenting in a submuscular or subgaleal location. They show a predilection for male adults.18,19 Lipoma arising in the orbit (orbital lipoma) is rare but may lead to exophthalmus and visual disturbances.20–22
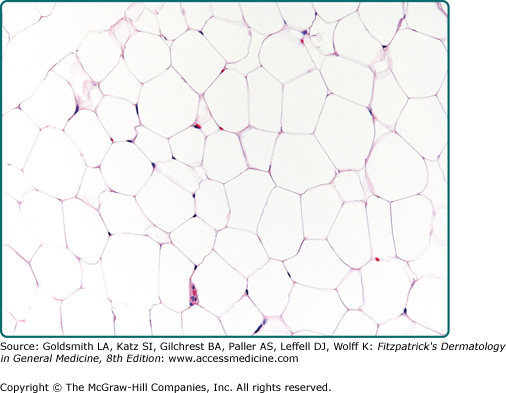
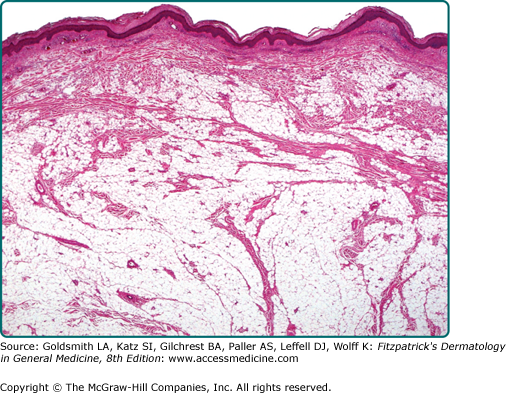
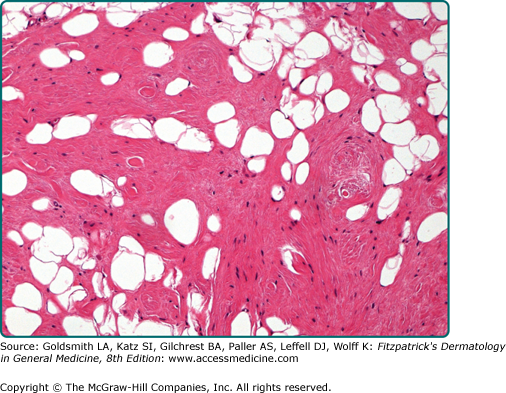
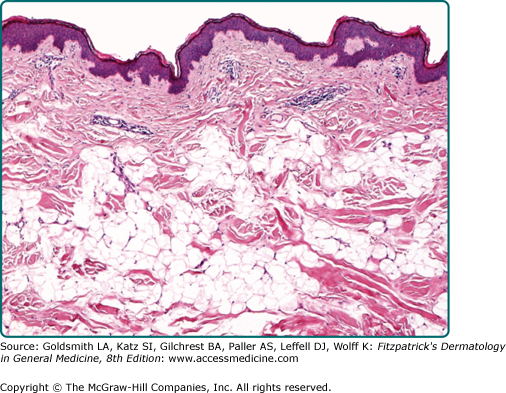
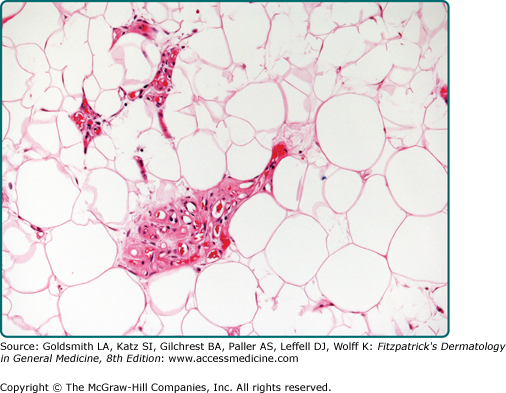
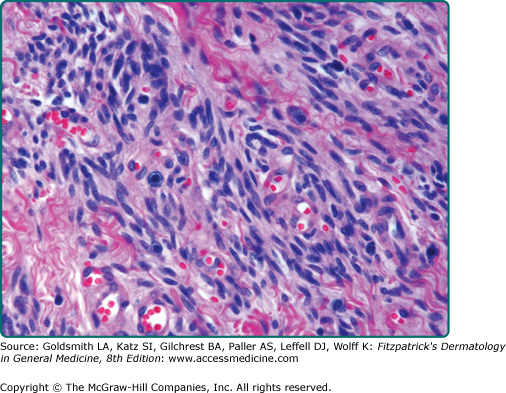
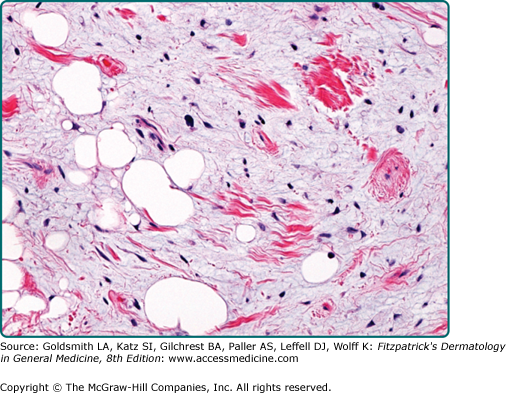
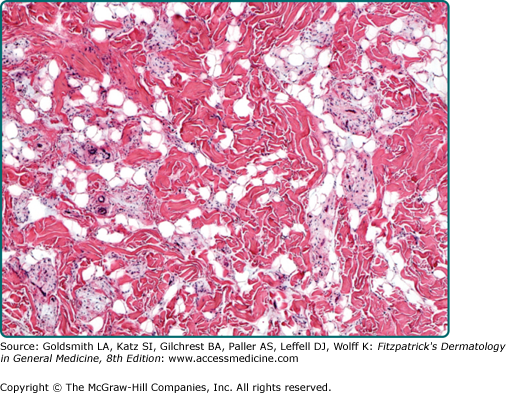
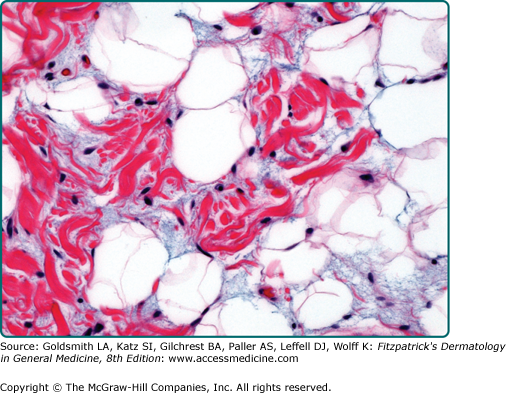
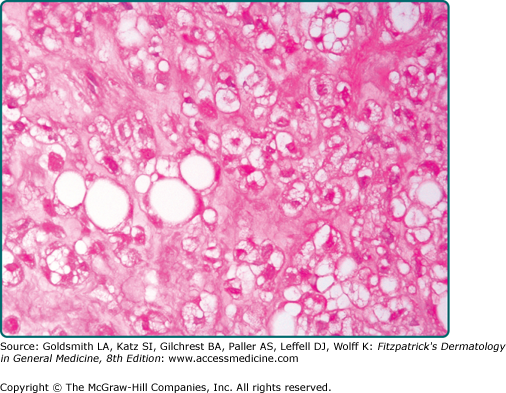
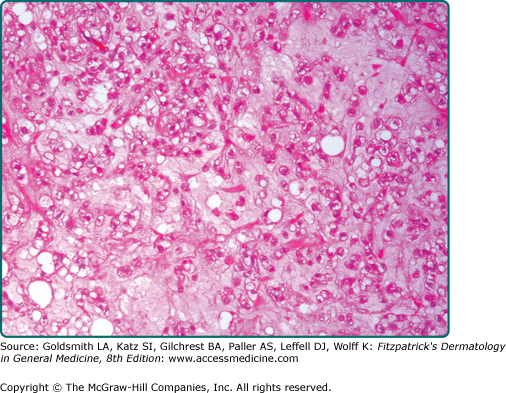
Conventional lipomas are circumscribed masses surrounded by a thin fibrous capsule. They are composed of lobules of mature white adipose tissue divided by delicate and inconspicuous fibrous septa containing thin-walled capillary-sized vessels (Fig. 129-2). The adipocytes are univacuolated and mature with eccentrically placed, compressed nuclei. There is only slight variation in adipocyte size, and nuclear atypia is not a feature. Morphologically, lipomas are indistinguishable from the surrounding adipose tissue and the identification of a distinct mass is necessary for the diagnosis. Lipomas may show changes of trauma with varying amounts of fat necrosis and inflammation. Extensive involvement of the dermis is known as dermal lipoma. These tumors are not encapsulated and are frequently less circumscribed than other forms of superficial lipoma (Fig. 129-3). Lipomas with increased fibrous tissue are referred to as fibrolipomas (Fig. 129-4). In contrast to atypical lipomatous tumors, cellularity is low within the fibrous strands, and no nuclear atypia is present. Myxolipomas are characterized by the presence of conspicuous myxoid stroma. Angiomyxolipoma or vascular myxolipoma is characterized by a myxoid stromal background in addition to a proliferation of vessels of variable sizes.23,24 A lipoma containing metaplastic bone or cartilage within the tumor is referred to as an osteolipoma or chondrolipoma, respectively. Cutaneous adenolipoma refers to the presence of intratumoral sweat ducts and sweat glands may be cystically dilated.25,26
Intramuscular lipoma can either present as a circumscribed intramuscular mass or show an infiltrative growth of adipocytes in between skeletal muscle fibers (Fig. 129-5).
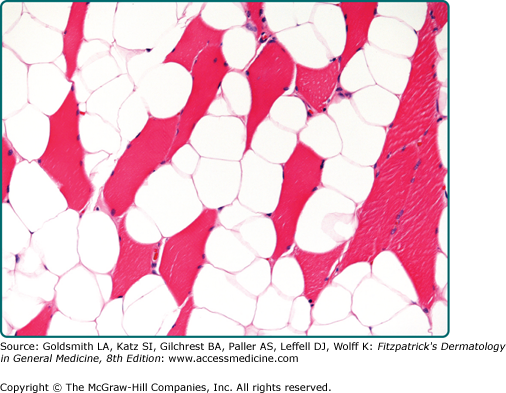
Lipomas are entirely benign tumors and, with the exception of intramuscular lipomas, local recurrence is rare. The infiltrative variant of intramuscular lipoma is associated with an approximately 19% chance of local recurrence, but metastasis does not occur.16
Lipomatosis
|
Diffuse lipomatosis 27,28 is characterized by overgrowth of adipose tissue involving subcutaneous tissue and skeletal muscle of the trunk and extremities. Osseous involvement may also be a feature. Young children are predominantly affected, but presentation may become apparent in adulthood. Tumors can grow to a large size, causing disfigurement and loss of function of the affected limb. Due to the diffuse growth of these tumors, complete excision may not be possible and recurrences are frequent.
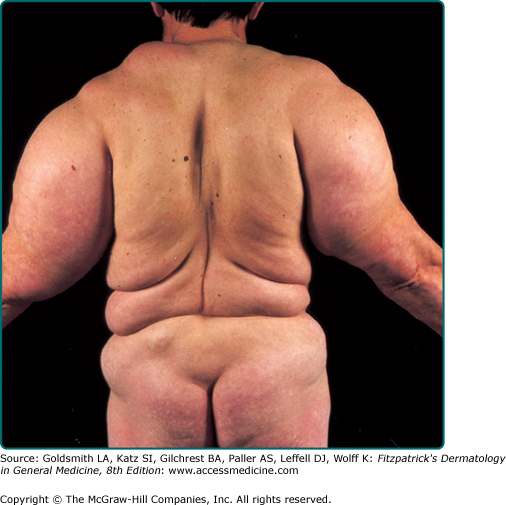
Benign symmetric lipomatosis (Madelung’s disease, multiple symmetric lipomatosis)29–36 is characterized by multiple symmetric masses composed of nonencapsulated adipose tissue with a predilection for the subcutaneous tissue and skeletal muscle of the neck, shoulder, and proximal upper limbs (Fig. 129-6). Presentation is in adulthood with a marked male predominance of 15:1. The estimated overall incidence is 1 in 25,000, with increased frequency in the Mediterranean region. The disease is associated with increased alcohol intake in the majority of cases. Two clinical variants are currently recognized. Type 1 disease is characterized by a symmetric distribution of adipose tissue, giving rise to a “pseudoathletic” appearance, whereas type 2 disease shows a more diffuse distribution, giving rise to a picture of more generalized obesity. An associated polyneuropathy affecting sensory, motor, and autonomic function is frequently present. The disease course is slowly progressive, and treatment is difficult due to infiltration of deep-seated structures and major nerves and vessels. There is significant disease-related mortality due to compression of vital structures as well as autonomic neuropathy with sudden cardiac death. Etiologically, the disease has been speculated to be a result of hypertrophy of brown fat due to a defect in adrenergic lipolysis.
Pelvic lipomatosis37–40 is an unusual proliferation of adipose tissue involving the pelvis and retroperitoneal space. The disorder is most common among men in the third and fourth decades, and blacks account for about two-thirds of cases. Urinary symptoms are frequent presenting signs, and the disease is associated with cystitis in 75% of cases. Obstructive uropathy and renal failure may be complications of the disease.
Adiposis dolorosa (Dercum’s disease)41–48 is rare and typically affects middle-aged women, although men may occasionally also be affected. The disease is typically sporadic, and familial cases are exceptional. There is an increased incidence with obesity. Patients present with multiple painful subcutaneous lipomatous lesions frequently associated with other symptoms such as weakness, depression, confusion, lethargy, or dementia. The disease predominantly involves the arms and trunk but may be progressive to involve large parts of the body. Treatment modalities include pain relief as well as surgical control with excision or liposuction. Weight reduction can be beneficial.
Human immunodeficiency virus lipodystrophy49–53 occurs in the setting of protease inhibitor treatment or other forms of antiretroviral therapy in patients with acquired immunodeficiency syndrome (see Chapter 198). There is a predilection for cervical fat pads, the breast, and visceral fat. Other associations include hyperlipidemia, insulin resistance, type 2 diabetes, and fat wasting affecting the face and limbs.
Lipomatosis of Nerve (Fibrolipomatous Hamartoma of Nerve)
|
 Lipomatosis of nerve is rare and affects predominantly infants and young children. Presentation at birth is not uncommon.54 It is only rarely seen in young adults.
Lipomatosis of nerve is rare and affects predominantly infants and young children. Presentation at birth is not uncommon.54 It is only rarely seen in young adults.
 Clinical presentation is as a slowly growing mass that may be associated with pain and paresthesia due to compression of the affected nerve. There is a strong predilection for the hand, including the wrist, palm, and fingers, and, less frequently, the foot. The median nerve and its branches followed by the ulnar nerve are most commonly affected.54 Involvement of cranial nerves and the brachial plexus has been reported but is exceptional.55,56 In a subset of patients, there may be accompanying overgrowth of bone resulting in macrodactyly.
Clinical presentation is as a slowly growing mass that may be associated with pain and paresthesia due to compression of the affected nerve. There is a strong predilection for the hand, including the wrist, palm, and fingers, and, less frequently, the foot. The median nerve and its branches followed by the ulnar nerve are most commonly affected.54 Involvement of cranial nerves and the brachial plexus has been reported but is exceptional.55,56 In a subset of patients, there may be accompanying overgrowth of bone resulting in macrodactyly.
 The lesions are characterized by a proliferation of adipose and fibrous tissue within the epineurium infiltrating along and in between nerve bundles. There is marked concentric fibrosis affecting both epineurium and perineurium.54 Metaplastic bone formation may rarely occur.57
The lesions are characterized by a proliferation of adipose and fibrous tissue within the epineurium infiltrating along and in between nerve bundles. There is marked concentric fibrosis affecting both epineurium and perineurium.54 Metaplastic bone formation may rarely occur.57
 The clinical behavior is entirely benign, but adequate treatment is difficult because of the anatomic location and involvement of major nerves.54
The clinical behavior is entirely benign, but adequate treatment is difficult because of the anatomic location and involvement of major nerves.54
Nevus Lipomatosus Superficialis
|
 Nevus lipomatosus superficialis is a rare form of connective tissue-type nevus that affects children and young adults in the first two decades of life. There is an equal gender distribution.58–62
Nevus lipomatosus superficialis is a rare form of connective tissue-type nevus that affects children and young adults in the first two decades of life. There is an equal gender distribution.58–62
 The classic presentation is as multiple papules and nodules that may coalesce to form larger plaques. There is a predilection for the buttocks, upper posterior thighs, and lumbar back. Occasionally, involvement may be extensive, and the lesions may form confluent linear plaques along the skinfolds. This phenomenon has been reported as the “Michelin tire man” appearance.63,64 Solitary lesions occur predominantly in adults and are more likely to represent a fibroepithelial polyp containing adipose tissue or an intradermal lipoma.
The classic presentation is as multiple papules and nodules that may coalesce to form larger plaques. There is a predilection for the buttocks, upper posterior thighs, and lumbar back. Occasionally, involvement may be extensive, and the lesions may form confluent linear plaques along the skinfolds. This phenomenon has been reported as the “Michelin tire man” appearance.63,64 Solitary lesions occur predominantly in adults and are more likely to represent a fibroepithelial polyp containing adipose tissue or an intradermal lipoma.
 The histologic features show mature adipose tissue in varying amounts within the superficial dermis (eFig. 129-6.1).
The histologic features show mature adipose tissue in varying amounts within the superficial dermis (eFig. 129-6.1).
Piezogenic Pedal Papules
 Piezogenic pedal papules are relatively common. Patients present bilaterally with painful, small papules and nodules in the heel area of the foot. The lesions occur during periods of standing, but disappear when pressure is relieved.65–67 Piezogenic pedal papules have also been reported on the wrist and are present in about a third of patients with Ehlers–Danlos syndrome.68,69 Etiologically, they are thought to be due to herniation of subcutaneous fat into dermis presumably due to connective tissue defects.
Piezogenic pedal papules are relatively common. Patients present bilaterally with painful, small papules and nodules in the heel area of the foot. The lesions occur during periods of standing, but disappear when pressure is relieved.65–67 Piezogenic pedal papules have also been reported on the wrist and are present in about a third of patients with Ehlers–Danlos syndrome.68,69 Etiologically, they are thought to be due to herniation of subcutaneous fat into dermis presumably due to connective tissue defects.
 Biopsy reveals a thickened dermis as well as loss of the normal compartmentalization of fat lobules in deep dermis and superficial subcutis. In addition, there is thinning or loss of subcutaneous fibrous septa.65
Biopsy reveals a thickened dermis as well as loss of the normal compartmentalization of fat lobules in deep dermis and superficial subcutis. In addition, there is thinning or loss of subcutaneous fibrous septa.65
Precalcaneal Congenital Fibrolipomatous Hamartoma
 Precalcaneal congenital fibrolipomatous hamartoma, also known as pedal papules in the newborn, is a poorly documented condition in the literature.70,71
Precalcaneal congenital fibrolipomatous hamartoma, also known as pedal papules in the newborn, is a poorly documented condition in the literature.70,71
 Presentation is usually at birth or within the first few month of life as bilateral symmetrical papules on the medial plantar aspect of the foot in a precalcaneal location. The skin-colored nodules are painless, measure approximately 1 cm in diameter, and are slowly enlarging.70,71
Presentation is usually at birth or within the first few month of life as bilateral symmetrical papules on the medial plantar aspect of the foot in a precalcaneal location. The skin-colored nodules are painless, measure approximately 1 cm in diameter, and are slowly enlarging.70,71

Angiolipoma
|
Subcutaneous angiolipomas are relatively frequent and typically occur in young adults in their teens and 20s, with a strong male predilection.72–74 They are rare in children and in the elderly.
Angiolipomas have traditionally been classified as adipocyte tumors. However, in contrast to most lipomas they appear to have a consistently normal karyotype, and it has been suggested that they may be reactive or hamartomatous rather than neoplastic.74 The fact that angiolipomas can occasionally be almost exclusively composed of blood vessels (cellular angiolipoma) has led to the speculation that they may in fact be hemangiomas rather than lipomas.74 There is an increased familial incidence, but no inheritance pattern has been elucidated as yet.75
A wide range of sites can be affected, but there is a predilection for the forearm followed by the trunk, upper arm, and legs.72–74 Angiolipomas are often multiple and present as subcutaneous nodules characteristically smaller than 2 cm. Tenderness and pain are frequently associated symptoms.
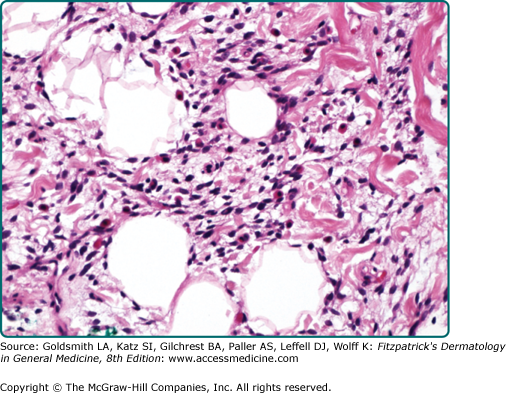
Angiolipomas are circumscribed and encapsulated. They show an admixture of mature fat and capillary-sized small branching vessels in varying proportions (Fig. 129-7 and eFig. 129-7.1). The vascular density is often increased at the periphery in a subcapsular distribution. Fibrin thrombi are typically encountered. The term cellular angiolipoma is applied to those lesions that are almost exclusively composed of vascular elements (eFig. 129-7.2).76–78
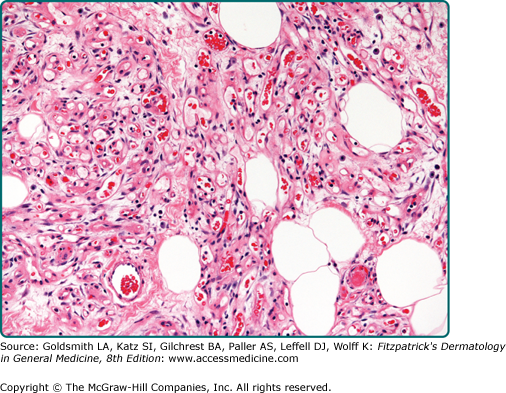
The appearances of angiolipoma are quite characteristic. The differential diagnosis of cellular angiolipoma includes vascular tumors such as Kaposi sarcoma, spindle cell hemangioma, and angiosarcoma.
Spindle Cell and Pleomorphic Lipoma
|
 Spindle cell lipoma and pleomorphic lipoma are believed to constitute a morphologic continuum. This view is based on the finding that there is significant clinical, histologic, and cytogenetic overlap and the fact that features of both can be present in a single lesion.79–87 These lipomas are rare; they represent only approximately 1.5% of all fatty tumors and are 60 times less frequent than conventional lipomas.80 They show a predilection for middle-aged to elderly adults (median age, 55 years) and a strong male predominance.79–87
Spindle cell lipoma and pleomorphic lipoma are believed to constitute a morphologic continuum. This view is based on the finding that there is significant clinical, histologic, and cytogenetic overlap and the fact that features of both can be present in a single lesion.79–87 These lipomas are rare; they represent only approximately 1.5% of all fatty tumors and are 60 times less frequent than conventional lipomas.80 They show a predilection for middle-aged to elderly adults (median age, 55 years) and a strong male predominance.79–87
 Spindle cell and pleomorphic lipomas show similar cytogenetic features. In comparison to conventional lipomas, their karyotype is more complex and frequently hypodiploid with frequent partial losses and few balanced rearrangements. Monosomy and partial losses involving chromosomes 13 and 16 are the most frequent findings.2,79,88–90
Spindle cell and pleomorphic lipomas show similar cytogenetic features. In comparison to conventional lipomas, their karyotype is more complex and frequently hypodiploid with frequent partial losses and few balanced rearrangements. Monosomy and partial losses involving chromosomes 13 and 16 are the most frequent findings.2,79,88–90
 Spindle cell and pleomorphic lipoma present as circumscribed, mobile masses, often with a long-standing history. They are small, measuring around 5 cm, and almost exclusively present on the posterior neck, shoulder, and upper back.79–87 Other anatomic sites in the head and neck region, including the oral cavity, can occasionally be affected.91 Rarely, these tumors are multiple and familial.92,93
Spindle cell and pleomorphic lipoma present as circumscribed, mobile masses, often with a long-standing history. They are small, measuring around 5 cm, and almost exclusively present on the posterior neck, shoulder, and upper back.79–87 Other anatomic sites in the head and neck region, including the oral cavity, can occasionally be affected.91 Rarely, these tumors are multiple and familial.92,93
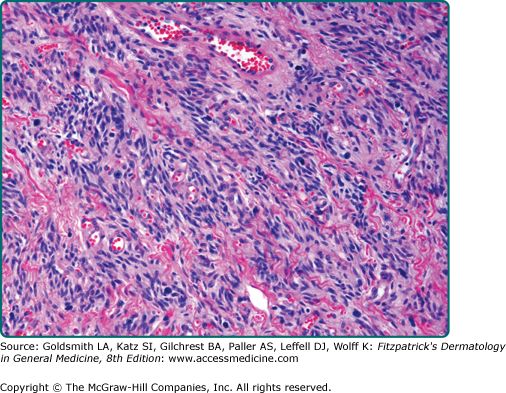
 Both tumors are circumscribed and are typically located within the subcutis. Spindle cell lipoma is characterized histologically by the presence of mature adipocytes admixed with bland-appearing and uniform, stubby spindle cells in a collagenous and myxoid stroma containing ropey collagen fibers and conspicuous mast cells (eFigs. 129-7.3, 129-7.4 and 129-7.5). Myxoid change can be prominent (eFig. 129-7.6), and occasionally slit-like spaces resembling vascular channels may be present (pseudoangiomatous variant).94 Mitotic activity is virtually absent. The characteristic feature of pleomorphic lipoma is the presence of bizarre multinucleate giant cells, termed floret cells. These cells show eosinophilic cytoplasm and multiple crowded and overlapping hyperchromatic nuclei arranged in a circle or semicircle resembling the petals of a flower (eFig. 129-7.7). As with spindle cell lipoma, there is a variably myxoid and collagenous matrix admixed with mature adipose tissue and containing spindled to rounded cells with hyperchromatic nuclei (eFig. 129-7.8). An inflammatory infiltrate may be present.
Both tumors are circumscribed and are typically located within the subcutis. Spindle cell lipoma is characterized histologically by the presence of mature adipocytes admixed with bland-appearing and uniform, stubby spindle cells in a collagenous and myxoid stroma containing ropey collagen fibers and conspicuous mast cells (eFigs. 129-7.3, 129-7.4 and 129-7.5). Myxoid change can be prominent (eFig. 129-7.6), and occasionally slit-like spaces resembling vascular channels may be present (pseudoangiomatous variant).94 Mitotic activity is virtually absent. The characteristic feature of pleomorphic lipoma is the presence of bizarre multinucleate giant cells, termed floret cells. These cells show eosinophilic cytoplasm and multiple crowded and overlapping hyperchromatic nuclei arranged in a circle or semicircle resembling the petals of a flower (eFig. 129-7.7). As with spindle cell lipoma, there is a variably myxoid and collagenous matrix admixed with mature adipose tissue and containing spindled to rounded cells with hyperchromatic nuclei (eFig. 129-7.8). An inflammatory infiltrate may be present.
 Occasionally, spindle cell as well as pleomorphic lipomas arise within the dermis. These dermal tumors have features similar to those described earlier but are less circumscribed and show an infiltrative growth between dermal collagen bundles (eFigs. 129-7.9 and 129-7.10).95 In contrast to subcutaneous lesions, intradermal examples show a wide anatomic distribution.
Occasionally, spindle cell as well as pleomorphic lipomas arise within the dermis. These dermal tumors have features similar to those described earlier but are less circumscribed and show an infiltrative growth between dermal collagen bundles (eFigs. 129-7.9 and 129-7.10).95 In contrast to subcutaneous lesions, intradermal examples show a wide anatomic distribution.
 By immunohistochemical analysis, the spindle cells express CD34 and rarely S100 protein.
By immunohistochemical analysis, the spindle cells express CD34 and rarely S100 protein.
 The differential diagnosis for spindle cell and pleomorphic lipomas includes the following:
The differential diagnosis for spindle cell and pleomorphic lipomas includes the following:
- Atypical lipomatous tumor
- Solitary fibrous tumor
- Cellular angiofibroma

Chondroid Lipoma
- Chondroid lipoma is a rare and benign tumor that affects adults and shows a female predominance.
- The anatomic distribution is wide, but there is a predilection for the proximal extremities and limb girdle.
- The unique histologic features include the presence of mature adipose tissue, lipoblasts, and a chondroid matrix.
 Chondroid lipoma is a relatively recently recognized and exceedingly rare benign lipomatous tumor.96 It shows a predilection for adults and a wide age distribution with a median of 36 years. There appears to be a significant female predominance (estimated at 1:4).96
Chondroid lipoma is a relatively recently recognized and exceedingly rare benign lipomatous tumor.96 It shows a predilection for adults and a wide age distribution with a median of 36 years. There appears to be a significant female predominance (estimated at 1:4).96
 Ultrastructural analysis confirms adipocyte rather than cartilaginous differentiation.97 Cytogenetically, a balanced translocation involving chromosomes 11 and 16, t(11;16)(q13;p12–13), has been shown in two separate tumors.98,99 The 11q13 locus has also been found to be involved in lipoma as well as hibernoma. However, rearrangements in these tumors are not associated with the 16p12–13 locus.
Ultrastructural analysis confirms adipocyte rather than cartilaginous differentiation.97 Cytogenetically, a balanced translocation involving chromosomes 11 and 16, t(11;16)(q13;p12–13), has been shown in two separate tumors.98,99 The 11q13 locus has also been found to be involved in lipoma as well as hibernoma. However, rearrangements in these tumors are not associated with the 16p12–13 locus.
 Chondroid lipoma is a relatively small tumor measuring approximately 5 cm. Larger examples of over 10 cm have also been reported. It presents as a painless circumscribed mass of variable duration and often comes to clinical attention because of a history of recent growth. The proximal extremities and limb girdles are the most frequently affected anatomic sites,96 but the trunk as well as the head and neck region, including intraoral sites, may also be affected.97,100–102 Tumors are typically deep-seated, involving deep subcutaneous tissue, fascia, and skeletal muscle.96 Imaging studies are rather nonspecific and show a multilobular and circumscribed mass containing fatty elements.102–104
Chondroid lipoma is a relatively small tumor measuring approximately 5 cm. Larger examples of over 10 cm have also been reported. It presents as a painless circumscribed mass of variable duration and often comes to clinical attention because of a history of recent growth. The proximal extremities and limb girdles are the most frequently affected anatomic sites,96 but the trunk as well as the head and neck region, including intraoral sites, may also be affected.97,100–102 Tumors are typically deep-seated, involving deep subcutaneous tissue, fascia, and skeletal muscle.96 Imaging studies are rather nonspecific and show a multilobular and circumscribed mass containing fatty elements.102–104
 The characteristic feature of chondroid lipoma is the admixture of a mature adipocyte component and a chondroid matrix containing lipoblasts.96 This well-circumscribed tumor is frequently encapsulated and multilobulated. It is composed of univacuolated and multivacuolated cells, occasionally with eosinophilic cytoplasm, showing cytologic features reminiscent of those of lipoblasts or chondroblasts (eFig. 129-7.11).96 These cells contain small lipid droplets as well as periodic acid-Schiff-positive glycogen.96 They are arranged in cords, nests, and strands as well as more solid areas set in a background of a chondroid matrix typically containing chondroitin sulfates (eFig. 129-7.12).105 Intricately admixed are variable amounts of mature adipose tissue. Tumors can be highly vascularized and show areas of hemorrhage, fibrosis, and calcifications.
The characteristic feature of chondroid lipoma is the admixture of a mature adipocyte component and a chondroid matrix containing lipoblasts.96 This well-circumscribed tumor is frequently encapsulated and multilobulated. It is composed of univacuolated and multivacuolated cells, occasionally with eosinophilic cytoplasm, showing cytologic features reminiscent of those of lipoblasts or chondroblasts (eFig. 129-7.11).96 These cells contain small lipid droplets as well as periodic acid-Schiff-positive glycogen.96 They are arranged in cords, nests, and strands as well as more solid areas set in a background of a chondroid matrix typically containing chondroitin sulfates (eFig. 129-7.12).105 Intricately admixed are variable amounts of mature adipose tissue. Tumors can be highly vascularized and show areas of hemorrhage, fibrosis, and calcifications.
 By immunohistochemical analysis, lipoblasts are positive for S100 protein. They are negative for epithelial membrane antigen and smooth muscle actin.105
By immunohistochemical analysis, lipoblasts are positive for S100 protein. They are negative for epithelial membrane antigen and smooth muscle actin.105
 Ultrastructural studies demonstrate intracytoplasmic lipid and glycogen as well as pinocytotic vesicles. These findings support adipocyte rather than cartilaginous differentiation.105
Ultrastructural studies demonstrate intracytoplasmic lipid and glycogen as well as pinocytotic vesicles. These findings support adipocyte rather than cartilaginous differentiation.105
 Differential diagnosis for chondroid lipoma includes the following:
Differential diagnosis for chondroid lipoma includes the following:
- Myxoid liposarcoma
- Extraskeletal myxoid chondrosarcoma

Myolipoma of Soft Tissue
 Myolipoma of soft tissue is also known as extrauterine lipoleiomyoma and is characterized by its admixture of mature adipocyte and smooth muscular components. It is an exceedingly rare tumor occurring in adulthood, with a female predominance of 2:1.106
Myolipoma of soft tissue is also known as extrauterine lipoleiomyoma and is characterized by its admixture of mature adipocyte and smooth muscular components. It is an exceedingly rare tumor occurring in adulthood, with a female predominance of 2:1.106
 Myolipomas can grow to a significant size and average 15 cm. They occur in deep soft tissue of the retroperitoneum, abdominal cavity, and inguinal area but can also arise within subcutaneous tissue of the trunk and extremities. Involvement of deep structures such as skeletal muscle and fascia is frequent. Myolipomas present as palpable masses but may be incidental findings when located at visceral sites.
Myolipomas can grow to a significant size and average 15 cm. They occur in deep soft tissue of the retroperitoneum, abdominal cavity, and inguinal area but can also arise within subcutaneous tissue of the trunk and extremities. Involvement of deep structures such as skeletal muscle and fascia is frequent. Myolipomas present as palpable masses but may be incidental findings when located at visceral sites.
 Myolipoma of soft tissue is a circumscribed and at least partially encapsulated neoplasm composed of mature adipose tissue with evenly distributed traversing fascicles of smooth muscle. It is important to note that there is no cytologic atypia or mitotic activity of either component, and thick-walled vessels as seen in angiomyolipoma are absent.
Myolipoma of soft tissue is a circumscribed and at least partially encapsulated neoplasm composed of mature adipose tissue with evenly distributed traversing fascicles of smooth muscle. It is important to note that there is no cytologic atypia or mitotic activity of either component, and thick-walled vessels as seen in angiomyolipoma are absent.
By immunohistochemical analysis, the smooth muscle component stains strongly and diffusely positive for smooth muscle actin and desmin.
The differential diagnosis for myolipoma of soft tissue includes the following:
- Liposarcoma
- Angiomyolipoma

Hibernoma
|
Hibernoma is a well recognized but rare benign adipocyte tumor that shows a wide age distribution. Young adults (mean age, 38 years) are predominantly affected, but presentation in the pediatric population as well as in the elderly is possible. Males appear to be affected only slightly more frequently than females.107
The etiology of this rare tumor is unclear. Karyotypes can be slightly more complex than those observed in other benign lipomatous tumors, but structural rearrangements involving chromosome band 11q13 appear to be reproducible.108–111
Hibernoma is a painless, slowly enlarging tumor affecting a wide range of anatomic sites. There appears to be a predilection for areas in which brown fat can be found physiologically, and presentation on the trunk, especially the scapular area, the shoulder, and the head and neck is common. However, curiously the thigh appears to be the single most frequently affected site.107 Hibernomas are typically located in subcutaneous tissue or skeletal muscle but may occasionally affect the abdominal cavity, retroperitoneum, or intrathoracic location.112
Presentation as multiple separate lesions is exceptional.113 The average size is around 10 cm, but larger tumors up to 24 cm are not unusual.107 Imaging studies reveal a well-demarcated lobulated and septated mass showing contrast enhancement and tissue attenuation intermediate between those of fat and skeletal muscle.114–117
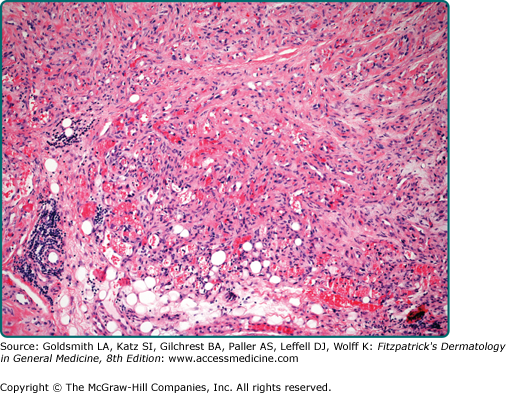
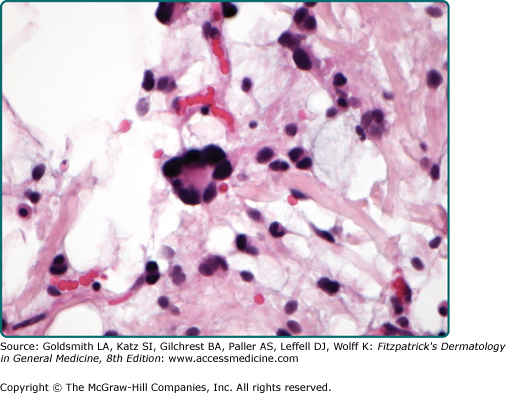
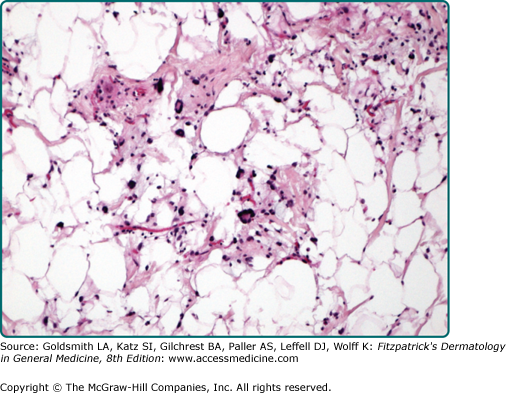
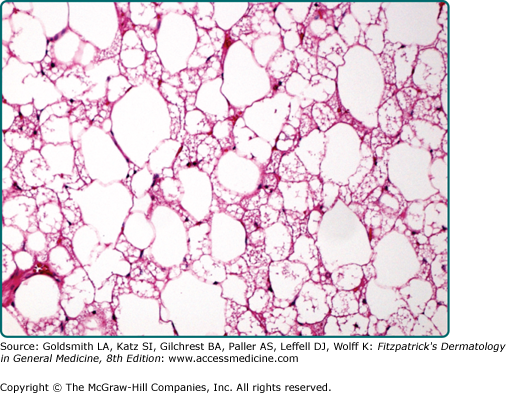
Hibernoma is a well-demarcated and lobulated neoplasm. The hallmark feature is its morphologic resemblance to brown fat. The tumors are composed of variable numbers of multivacuolated adipocytes with small, centrally placed nuclei and pale to eosinophilic and granular cytoplasm (eFig. 129-7.13). On the basis of the appearance of these brown fat cells, the quality of intervening stroma, and the presence of a spindle cell component, six histologic variants are recognized.107
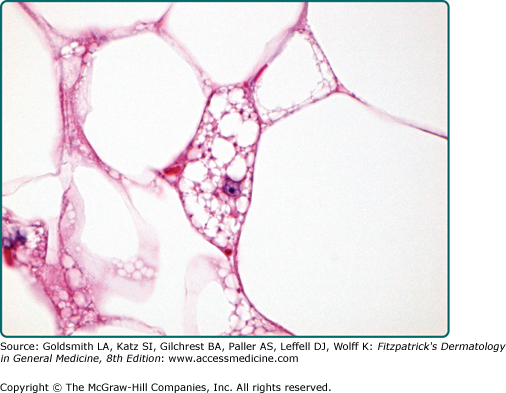
The typical variant is the most frequently encountered form and is characterized by large numbers of brown fat cells admixed with mature white fat (Fig. 129-8). Those tumors composed almost exclusively of brown fat cells with palely staining cytoplasm are further subclassified as the pale cell subtype. Tumors are labeled eosinophilic subtype when at least 50% of brown fat cells contain a deeply eosinophilic and granular cytoplasm. The mixed subtype is intermediate between the two and shows a roughly equal distribution of eosinophilic and pale-staining brown fat cells. Myxoid, lipoma-like, and spindle cell variants exist.
Hibernomas showing acellular myxoid areas of the intervening stroma are recognized as the myxoid variant. This variant affects predominantly men and presents in the head and neck and shoulder area.
The lipoma-like variant shows large areas of white fat differentiation with only scattered hibernoma cells lying in between.
The least frequent is the spindle cell variant, showing overlapping features of spindle cell lipoma and hibernoma. Areas of brown fat are admixed with the short and bland spindle cells typical of spindle cell lipoma, and ropey collagen bundles, myxoid stroma, mast cells, and mature white fat are also present. As with spindle cell lipoma, this variant presents in the posterior neck and scalp.
By immunohistochemical analysis, hibernomas stain positively for S100. CD34 expression is seen in the spindle cells of the spindle cell variant of hibernoma.107








