Abstract
Nail surgery is often feared by patients because of concerns regarding pain, both from injection of the local anesthetic and postoperatively, as well as the risk of permanent nail dystrophy. Potential dystrophic sequelae are also a concern for the clinician. A thorough working knowledge of nail anatomy, anesthetic techniques, and surgical procedures is a prerequisite for successful nail surgery. The goal is minimal pain and minimal scarring. It is also essential to involve a dermatopathologist who is familiar with the histologic idiosyncrasies of the nail unit.
Keywords
nail, nails, nail anatomy, nail anesthesia, nail biopsy, nail surgery, nail tumors
- ▪
A thorough understanding of the anatomy and physiology of the nail unit is a prerequisite for performing successful nail surgery
- ▪
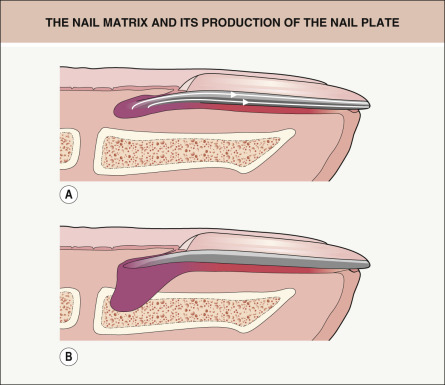
The nail matrix forms the nail plate; any damage to the matrix (including from surgical procedures) can cause permanent nail dystrophy
- ▪
Because there is no subcutaneous tissue in the nail unit, the dermis of the nail bed sits on the periosteum of the distal digit
- ▪
Preoperative evaluation prior to nail surgery is essential and should include appropriate diagnostic imaging
Introduction
An accurate diagnosis of nail disorders often requires clinicopathologic correlation. When performing a biopsy of the nail unit, it is important that: (1) the most appropriate surgical procedure be performed correctly; (2) there is precise handling of the specimen in the histopathology laboratory; and (3) a dermatopathologist with knowledge of the nuances of nail pathology examine the tissue . A range of disorders require nail surgery, from nail tumors to ingrown toenails. As with surgical procedures performed elsewhere, the major goals include establishing a diagnosis and/or providing treatment safely and with minimal pain or scarring . Because dermatologists are the physicians who understand and manage nail disorders, they are well suited to perform nail surgery. A solid grasp of the anatomy and physiology of the nail unit is a prerequisite for successful nail surgery. Additional requirements for an optimal outcome include a well-prepared patient, adequate anesthesia, proper surgical technique, and hemostasis ( Table 149.1 ).
| PREREQUISITES FOR SUCCESSFUL NAIL SURGERY |
|
Surgical Anatomy of the Nail Unit
Basic Anatomy
The components of the nail unit are the nail plate, the nail matrix, the nail bed, the hyponychium, and the proximal and lateral nail folds.
The nail matrix rests on the midportion of the distal phalanx and has a broad crescent shape ( Fig. 149.1 ). It is covered in large part by the proximal nail fold. On the great toe, the lateral horns of the matrix can extend as far as the midline of the lateral aspect of the digit or even farther ( Fig. 149.2 ). This is an important concept, especially when approaching longitudinal melanonychia that is localized primarily to the distal matrix or when performing a phenol matricectomy for ingrown nails. The distal portion of the nail matrix is sometimes visible through the proximal nail plate as the white half-moon-shaped structure called the lunula. While the proximal portion of the matrix produces the upper third of the nail plate, the distal portion provides the lower two-thirds (see Fig. 149.2 ). Consequently, surgery involving the distal matrix has a very low risk of producing nail dystrophy, as the upper layers of the nail plate will cover the defect .
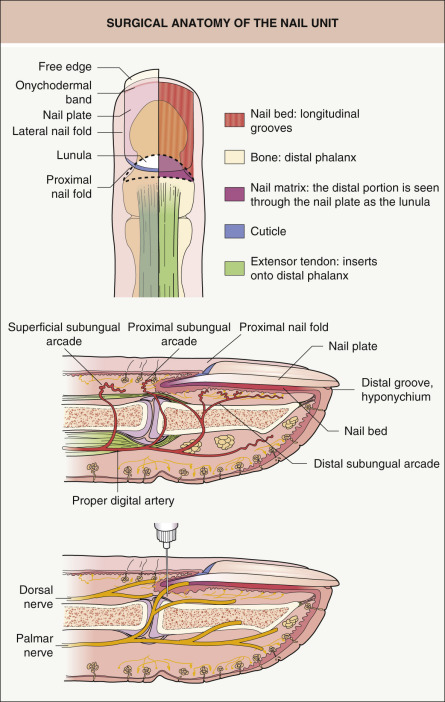
The nail bed , sometimes referred to as the sterile matrix, extends from the distal lunula to the hyponychium. A rich vascular supply leads to the pink color that is visible through the translucent nail plate. The nail bed is composed of longitudinal ridges and grooves which interlock with opposing structures on the undersurface of the nail plate. This explains the tight adhesion of the plate to the bed. Surgery of the nail bed rarely leads to permanent dystrophy of the nail apparatus, but it may result in mild onycholysis. An important feature of the nail bed is that there is no subcutaneous tissue beneath it. The dermis of the nail bed sits directly on the periosteum of the distal digit. The lack of subcutaneous tissue in the nail unit explains why nail surgical specimens should extend to the level of the periosteum.
The hyponychium begins at the most distal part of the nail bed, where the nail plate detaches to form its free edge and just proximal to the distal groove, and then it becomes contiguous with the volar skin of the digit. The hyponychium seals and protects the nail unit from environmental factors. Disruption of the hyponychium by trauma or disease can result in onycholysis, followed by bacterial and fungal contamination.
The proximal nail fold covers and protects most of the matrix and the newly formed plate. The most distal portion of the proximal nail fold gives rise to the cuticle, which adheres tightly to the proximal nail plate, thereby sealing and protecting the nail pocket from environmental pathogens and irritants.
The lateral folds ensheath the lateral aspects of the plate. Proximally, they merge with the proximal nail fold and distally with the hyponychium. The proximal and lateral nail folds are collectively called the paronychium. The term perionychium refers to the paronychium plus the hyponychium and nail bed .
The insertion of the extensor tendon of the digit onto the phalanx is just proximal to the most proximal portion of the matrix. In an adult, this is ~12 mm proximal to the cuticle. Except in the most extensive nail surgical procedures such as nail unit ablation, this tendon is not observed within the surgical field.
Innervation
Paired palmar and dorsal nerves course along the lateral sides of the digit in close approximation to the digital arteries (see Fig. 149.1 ). In general, the index, middle and ring fingertips get their innervation from the palmar digital nerves whereas the thumb and little (fifth) finger are innervated by the dorsal nerves . This is an important consideration when performing a digital block.
Vascular Supply
The paired proper digital arteries, which run along the lateral and volar sides of the digit, comprise the main blood supply to the nail unit (see Fig. 149.1 ). They anastomose to form three arcades: (1) the superficial arcade – supplies the area overlying the distal interphalangeal (DIP) joint; (2) the proximal arcade – supplies the proximal nail fold and matrix; and (3) the distal arcade – supplies the nail bed and hyponychium.
Preoperative Evaluation and Patient Preparation
A thorough and efficient preoperative evaluation is required prior to nail surgery. Screening for underlying diseases, especially those that predispose to peripheral vascular disease (e.g. diabetes mellitus, Raynaud phenomenon, atherosclerosis), should be done, in addition to a review of medications, allergies (e.g. povidone-iodine, antibiotics, narcotics, anesthetics, latex), smoking history, and past surgical procedures, in particular the presence of prosthetic heart valves and joint replacements (see Table 151.2 ). Physical examination should include inspection of all 20 nails as well as palpation of peripheral pulses. Appropriate laboratory tests for bacteria, fungi, and/or viruses should be obtained when there is a possibility of infection. Diagnostic imaging can detect underlying bony defects as well as define space-occupying lesions and their anatomic relationships prior to nail surgery. A full “procedure, alternatives and risks” (PAR) discussion should include the possibility of bleeding, pain, infection, and permanent nail dystrophy. Information regarding work disruption should be provided. Premedication is not particularly useful, except in those who are very anxious. No systemic drugs, including anticoagulants and antiplatelet agents, need to be discontinued . Prophylactic antibiotics are only indicated for individuals with high-risk cardiac conditions or prosthetic joint replacements at high risk for infection (see Tables 151.2 & 151.3 ). While not mandatory, clinical photographs of the preoperative nail may prove worthwhile. The digit is then prepped with alcohol, chlorhexidine, or povidone-iodine and sterilely draped.
Anesthesia of the Nail Unit
The choice of anesthetic will depend on the pain expected postoperatively. Plain 1% or 2% lidocaine and ropivacaine (2 mg/ml) have a more rapid onset while 0.5% bupivacaine provides adequate anesthesia after 15 minutes; there is a longer duration of anesthesia with the latter two local anesthetics (see Ch. 143 ). Although the dogma used to be an avoidance of epinephrine (adrenaline) in digital blocks, multiple studies involving thousands of patients support the premise that lidocaine with epinephrine can be safely injected into digits, as long as patients have no history of peripheral vascular compromise and the recommended volume is injected (see below) . However, as nail surgery is usually performed with a tourniquet, there is little need for the vasoconstrictive effect of epinephrine.
Pain during anesthesia comes from several factors: the needle prick, rapid injection, and acidity of the anesthetic. In order to reduce these side effects, the surgeon should use thin needles (30-gauge), inject very slowly, and buffer the lidocaine (see Ch. 143 ).
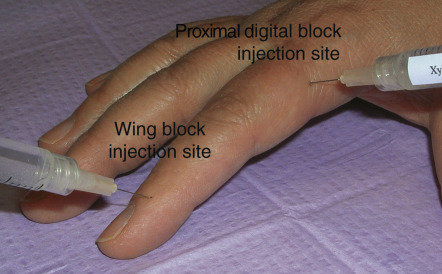
Anesthesia can be administered as a proximal digital block (ring block) or a distal digital block (wing block). For a ring block , 2–3 ml of 1% or 2% plain lidocaine is injected superficially into the base of the digit on each of its lateral sides ( Fig. 149.3 ). To prevent vasospasm and tamponade of the blood vessels, the volume of local anesthetic should be <1–1.5 ml on each side of the digit. The block is achieved within 15 to 20 minutes. This procedure may injure the neurovascular bundles at the base of the finger and therefore the authors prefer to use a distal block. In the distal digital block , the needle is inserted vertically, 1 cm lateral and proximal to the junction of the proximal and lateral folds; here 0.5 ml of the anesthetic is injected in order to anesthetize the dorsal nerve branch (see Fig. 149.3 ). The needle is then advanced vertically towards the palmar surface, where an additional 0.5 ml is injected around the palmar nerve branch (see Fig. 149.1 ). The procedure is then repeated on the opposite side to obtain full anesthesia of the nail unit. The wing block has several advantages over the proximal digital block: (1) the onset of action is quicker; (2) less volume of anesthetic is required; and (3) the injection is more comfortable. Injecting a longer-acting anesthetic (e.g. bupivacaine) as a wing block provides prolonged anesthesia and reduces bleeding after removal of the tourniquet due to the extra liquid-based pressure on the lateral digital arteries .
Instruments for Nail Surgery
Most of the instruments used in nail surgery are standard instruments used in cutaneous surgery. A few specific instruments are needed in order to make nail surgery easier to perform. An elevator allows atraumatic detachment of the plate from the bed and several types are available, e.g. Freer septum elevator, Locke elevator ( Fig. 149.4 ). Nail nippers are essential for cutting the nail plate. When cutting thick nails, the dual-action nail nipper is invaluable. The English nail splitter is very popular, but has a major drawback: its thicker lower jaw induces lateral onycholysis ahead of the cutting line. Straight nail nippers with their sharp, thinner, beveled jaws are less traumatic ( Fig. 149.5 ).


As nail surgery requires a bloodless surgical field, a tourniquet, applied for a maximum of 30 minutes, is very useful. Several options are available. The Penrose drain, clamped with a sturdy hemostat, is commonly used but studies have shown that it delivers high and unreliable pressure that has the potential for lateral nerve damage, and thus it is not recommended for digits. The best tourniquet is a sterile glove, half a size smaller than the adequate size. One fingertip of the glove is pierced with scissors and rolled back to the base of the proximal phalanx ( Fig. 149.6 ). This technique exsanguinates the digit and delivers reliable pressure under 500 mmHg. The remainder of the glove serves as a sterile field .

Nail Plate Avulsion
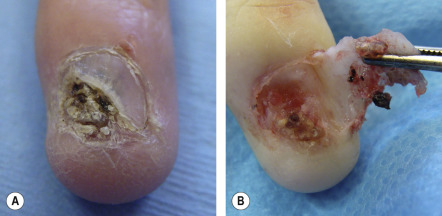
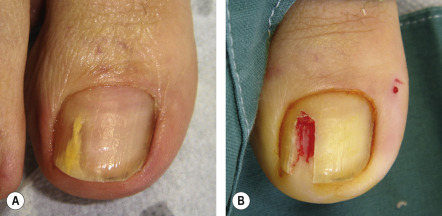
Nail avulsion is the most basic procedure in nail surgery and is a prelude to most other nail unit procedures. It allows visualization of the nail bed and matrix, thus providing good exposure for biopsy or excision ( Fig. 149.7 ). Total nail avulsion should be discouraged because as the counterpressure exerted by the nail plate disappears, the distal wall and the pulp raise upward in combination with a shrinkage of the nail bed. The result is more bulky soft tissue at the end of the digit and an increased risk of distal embedding during nail regrowth. Partial nail avulsion is therefore preferred , with the advantage being that a large portion of normal nail plate is left intact, reducing the risk of distal embedding . Partial nail avulsion serves as an adjuvant therapeutic intervention in onychomycosis as it reduces the fungal mass, especially of a dermatophytoma ( Fig. 149.8 ). In addition, nail avulsion is an early step in chemical matricectomy (see below), may be performed to drain an acute paronychia, and is a must when exploring pigmented lesions within the nail matrix. There are two approaches to nail avulsion – distal and proximal, although the latter is rarely used.
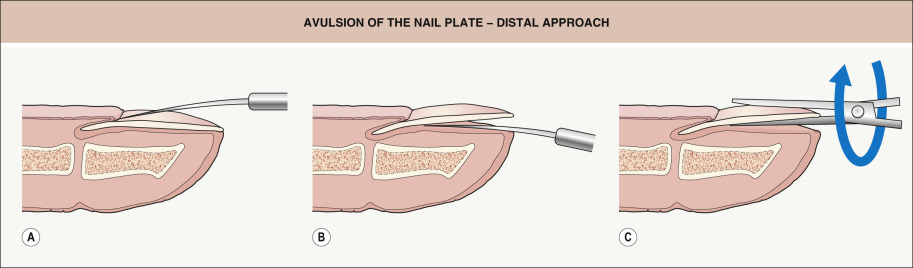
For distal nail plate avulsion , an elevator is first pushed under the proximal nail fold and slid back and forth from one side to the other in order to detach the fold from the plate ( Fig. 149.9A ). The elevator is then inserted under the free edge of the nail plate in a distal to proximal direction to free the plate from its bed ( Fig. 149.9B ). As the instrument reaches the matrix area where the attachment of the nail plate is looser, a decrease in resistance is felt. To loosen the entire plate, the instrument is inserted under the plate at several sites, advancing from the hyponychium to the matrix. Lateral motions across the nail bed should not be done to loosen the nail plate as this can injure the fragile longitudinal nail bed ridges. The plate is then grasped on one lateral edge by a hemostat or a nail puller and rotated ( Fig. 149.9C ) and pulled off the nail bed.
If the avulsion is performed to explore the entire matrix area, avulsion alone will not suffice. Two releasing incisions, ~1 cm in length, are made at each junction of the proximal and lateral nail folds, angling laterally and proximally ( Fig. 149.10 ). This allows the nail fold to be reflected so that the matrix can be inspected. When performing a biopsy or excisional surgery, skin hooks or sutures help to maintain the reflection of the proximal nail fold. At the end of the procedure, the fold is placed back into its original position and secured with simple interrupted sutures or cyanoacrylate adhesive. The nail plate, if not needed for pathologic examination or culture, should be repositioned to cover and protect the wound during the early stages of the healing process. It can be secured by sutures or adhesive. Although the plate will not reattach and is eventually shed, it provides protection and minimizes discomfort during the immediate postoperative period.

Biopsy Techniques
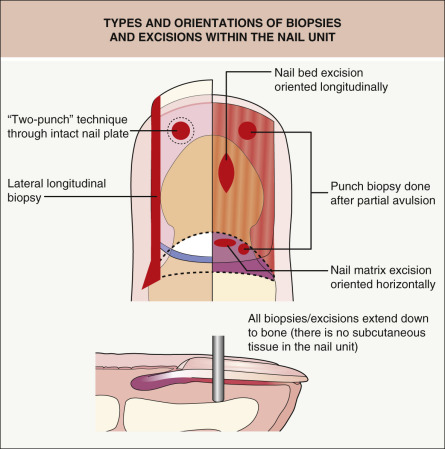
To minimize scarring and offer the best functional and cosmetic outcome, nail surgical procedures should follow a few rules. Within the nail bed, the incision should be oriented longitudinally, whereas within the matrix it should ideally be oriented horizontally ( Fig. 149.11 ). The surgical approach depends upon the location of the pathology within the nail unit.
Nail Bed Biopsy
Nail bed biopsy is a simple and safe technique that facilitates the diagnosis of a variety of nail bed disorders, from onycholysis to tumors ( Table 149.2 ). The nail plate is usually partially avulsed prior to the nail bed biopsy ( Fig. 149.12A ); however, occasionally the biopsy is performed through the nail plate. In the latter situation, the “two-punch” technique, in which a larger diameter punch biopsy instrument is used to create a circular defect in the nail plate then a smaller diameter instrument is used to obtain the nail bed biopsy specimen, can make removal of the nail bed tissue easier. The trephine should be advanced until there is contact with bone (see Fig. 149.11 ). If it is necessary to perform a punch biopsy >4 mm, the defect should be sutured closed in order to avoid secondary onycholysis. The nail bed is very fragile and reapproximation of the margins may be difficult. Nonetheless, it is amazing how very large defects of the nail bed (e.g. after Mohs surgery) may regenerate totally by second intention .
| CLINICAL FEATURES OF NAIL BED DISORDERS IN WHICH A BIOPSY MAY FACILITATE DIAGNOSIS AND SUBSEQUENT TREATMENT | |
|---|---|
| Diagnosis | Clinical features |
| Malignant tumors of the nail bed | |
| Squamous cell carcinoma, Bowen disease | Hyperkeratosis, dyschromia, onycholysis, destruction of the nail plate |
| Keratoacanthoma | Multiple or solitary, nail plate destruction, mass, erosion, granulation tissue, ± pain |
| Melanoma | Pigmentation of the nail bed, erosion, destruction of the nail plate; 25% are amelanotic |
| Metastatic carcinomas | Mass, pseudo-clubbing, nail dystrophy, dusky red color, ± pain |
| Kaposi sarcoma | Pigmentation, elevation, destruction of the nail plate |
| Basal cell carcinoma | Rare, variable clinical appearance |
| Benign tumors of the nail bed | |
| Pyogenic granuloma | Exuberant friable mass, needs to be distinguished from amelanotic melanoma |
| Glomus tumor | Spontaneous pain, blue–red mass |
| Epidermoid cyst | Mass, nail plate deformity |
| Fibroma | Mass, elevation, distortion of the nail (if presses on matrix, distal groove; if underneath nail plate, elevation of plate) |
| Exostosis | Mass, elevation of the nail plate, tenderness, secondary infection can occur |
| Osteochondroma | Enlargement of digit, elevation or destruction of the nail plate |
| Enchondroma | Mass, alteration of the nail plate, pain |
| Infectious conditions of the nail bed | |
| Onychomycosis | Hyperkeratosis, dyschromia, nail dystrophy, onycholysis |
| Warts | Verrucous mass, sometimes painful, nail plate deformity or destruction, must distinguish from verrucous or squamous cell carcinoma |
| Subungual scabies | Hyperkeratosis of hyponychium |
| Inflammatory dermatoses involving the nail bed | |
| Psoriasis | Onycholysis, hyperkeratosis, splinter hemorrhages, oil drop discoloration |
| Lichen planus | Violaceous discoloration, atrophy of nail bed; if nail matrix is involved, trachyonychia, hapalonychia (soft nails), dorsal pterygium |
| Other nail bed conditions | |
| Hemorrhage, trauma | Red–violet to black discoloration under nail plate; persistent or non-migrating discoloration needs to be distinguished from melanoma |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


