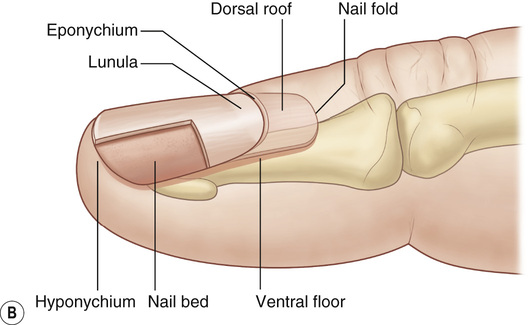
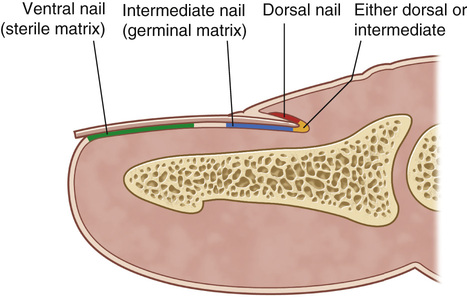
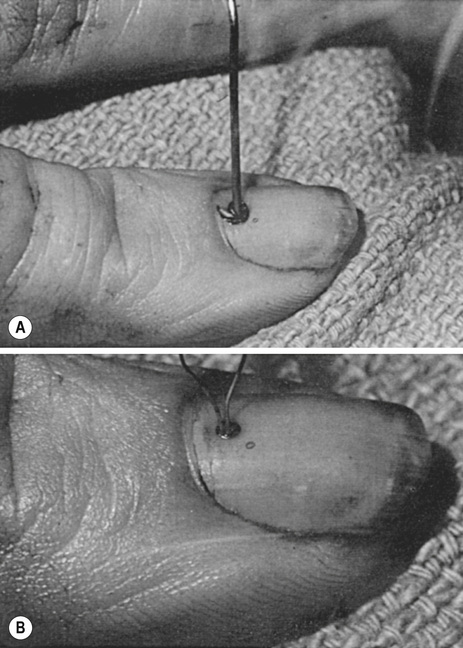
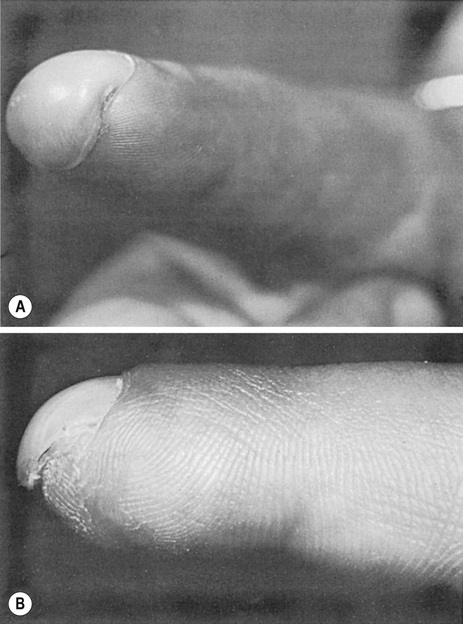
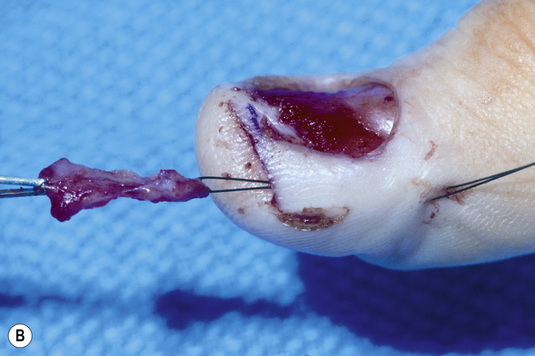
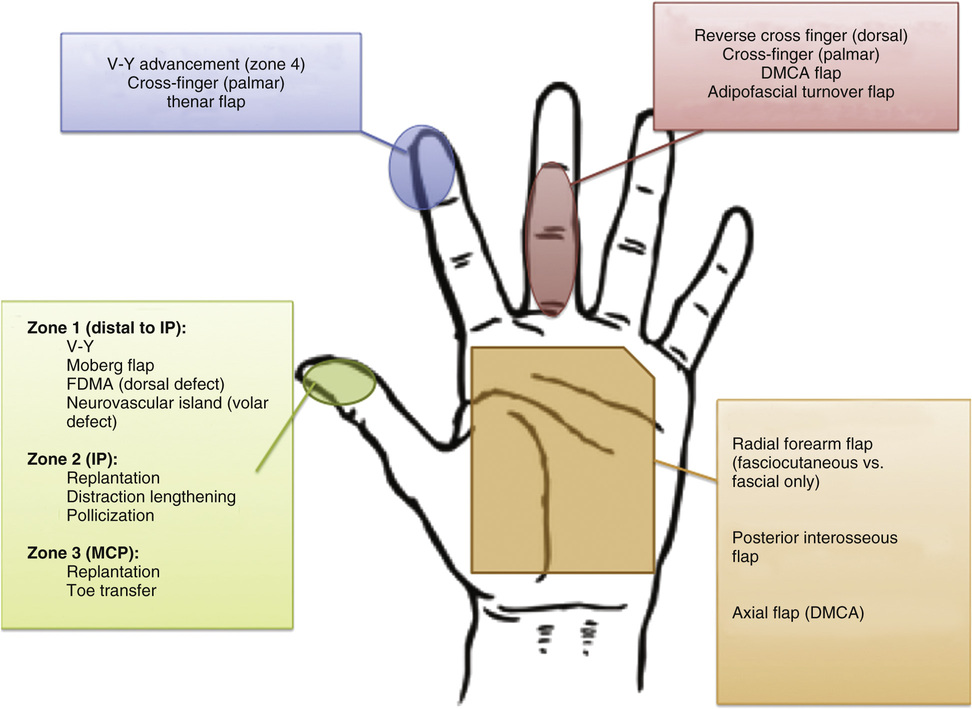
1. Perionychium • Nail bed • Surrounding skin (nail fold, paronychium, hyponychium) 2. Paronychium: The lateral skin that surrounds the nail bed and nail 3. Hyponychium: The skin and keratin along the distal edge of the nail bed 4. Eponychium: The skin proximal and dorsal to the nail fold 6. Matrix: The nail-plate growth centers ▪ Accounts for almost 90% of nail-plate production ▪ Soft tissue deep to nail plate at lunula and nail fold ▪ Accounts for 10% of nail production ▪ The soft tissue located deep to the nail plate, distal to the lunula/germinal matrix ▪ Responsible for adherence of nail plate to nail bed (see Figure 17.1) 1. Nail-plate growth is estimated to be 3 to 4 mm per month; complete nail-plate growth takes ~6 months. 3. Nail growth occurs in the germinal matrix, sterile matrix, and dorsal roof of the nail fold. • The dorsal roof of the nail fold produces nail-plate cells similar to those of the germinal matrix and has a significant role in producing the shiny appearance of the nail (see Figure 17.2). • Most commonly caused by crush injury • Signs: Pain and bleeding underneath nail with discoloration, signifying an injury to the nail bed ▪ >50% of the nail involved or disruption of the nail edges: Nail-plate removal and nail-bed repair (see Figure 17.3) • Commonly associated with distal phalanx fractures • Treatment: Nail-plate removal with nail-bed repair ▪ If distal phalanx fracture is present, it may require management. • Nail-bed repair can be performed with 6-0 absorbable sutures or 2-octylcyanoacrylate (Dermabond). • After repair, splint the eponychial fold to prevent fold adhesions and obstruction of nail growth. ▪ Can be performed with the original nail plate, aluminum foil, or nonadherent gauze 3. Complications of nail-bed injury ▪ Most common nail deformity after trauma ▪ Secondary to nail-bed scarring ▪ Secondary to inadequate bony support from the dorsal tuft of the distal phalanx ▪ Nail growth hooks volarly over the fingertip ▪ Treatment: Removal of redundant nail bed or advancement flap of volar fingertip tissue with no tension (see Figure 17.4) ▪ Treatment: Elevation of the nail plate with dermal grafting (see Figure 17.5) ▪ Scarred nail matrix after injury ○ Germinal matrix scar: Excision of scar tissue, full-thickness matrix graft from second toe ○ Sterile matrix scar: Excision of scar tissue, split-thickness matrix graft from second toe 1. In general, treatment options depend on wound size, location and orientation of injury, and presence or absence of exposed critical structures (e.g., bone, tendon, vasculature). • Volar soft-tissue loss ≤1 cm2: Secondary intention ▪ May have superior restoration of sensation and function compared to other options • >1-cm defect, without exposed bone or tendon: Skin graft ▪ Full-thickness grafts give better restoration of sensation. ▪ Split-thickness grafts will contact more, which may be advantageous in certain instances. • Large defects or defects with exposed tendon or bone: Local flaps (see Figure 17.6)
Nail-Bed Injuries, Soft-Tissue Amputations, and Replantation
General Fingernail and Nail-Bed Anatomy
Nail Growth and Physiology
Nail-Bed Injuries
Fingertip Soft-Tissue Injuries
Nail-Bed Injuries, Soft-Tissue Amputations, and Replantation
Chapter 17