Identification and classification of a patient’s skin lesions are important steps in the diagnosis of any skin disorder. The numerous descriptive terms used in dermatology can be overwhelming and at times confusing as there are some variations in the use and meaning of these words in the literature.1 However, a few simple terms can be used to describe the cutaneous findings in most skin diseases. Using proper terminology to describe skin findings is essential for both documentation and communication with other clinicians. The effort to use precise descriptive terms also encourages a clinician to look with more care and more closely at a patient’s skin lesions. The key features of skin lesions are (1) the type of lesion, (2) secondary changes to the surface of the lesion, (3) the color of the lesion, (4) the shape of the lesion, and (5) the arrangement and distribution of the lesions.
The first step is categorization of the primary skin lesion(s). This may be difficult if the lesions are excoriated or if the examination takes place late in the disease process. The lesion may need to be lightly touched or deeply palpated to accurately assess its features. Table 2-1 lists the 10 most common morphological terms for types of skin lesions. These are based on:
Diameter of the lesion.
Relationship of the lesion to the surface of the skin—is the lesion flat or elevated above the surface of the skin?
Composition of the lesion—is it fluid filled or solid?
| Terminology | Diameter | Morphology | Example |
|---|---|---|---|
Macule Patch | <0.5 cm >0.5 cm | Flat, level with surface of skin | Tinea versicolor (Figure 2-1) |
Papule Plaque | <0.5 cm >0.5 cm | Solid, elevated lesion | Dermatitis (Figure 2-2) |
| Wheal | Any size | White to pink edematous papule or plaque that lasts less than 24 h | Urticaria (Figure 2-3) |
| Nodule | >0.5 cm | Dermal or subcutaneous solid, elevated lesion | Amelanotic melanoma (Figure 2-4) |
Vesicle Bulla | <0.5 cm >0.5 cm | Blister containing fluid or blood | Pemphigus vulgaris (Figure 2-5) |
| Pustule | <0.5 cm | Cavity filled with pus, may be sterile | Pustular psoriasis (Figure 2-6) |
| Cyst | >0.5 cm | Cavity filled with pus or keratin | Epidermal cyst (Figure 2-7) |







Most textbooks use a lesion diameter of either 0.5 or 1 cm to distinguish between various lesion types. This textbook uses 0.5 cm. It is not uncommon for a skin disease to have multiple types of lesions. Therefore, terms such as maculopapular or vesiculobullous are commonly used.
Some lesions have a smooth surface, but surface changes frequently quickly develop during the course of a skin disorder. Table 2-2 lists common surface changes. Papulo-squamous is a term used to describe papules/plaques that have scale.
| Terminology | Surface Changes in Lesions | Example |
|---|---|---|
| Scale | Loose or adherent flake composed of stratum corneum cells. The term hyperkeratotic is used for small areas of thick adherent scale | Psoriasis (Figure 2-8) |
| Crust | Yellow, brown, black, or green surface deposits of serum, pus, and/or blood | Pemphigus vulgaris (Figure 2-9) |
| Lichenification | Thickening of the epidermis with accentuation of skin markings | Atopic dermatitis (Figure 2-10) |
| Fissure | Linear, sharply defined, deep crack in the skin | Callous (Figure 2-11) |
Erosion Excoriation | Localized loss of the superficial epidermis Linear or punctate, superficial, erosions in the skin caused by fingernails and sharp objects | Drug rash (Figure 2-12) |
| Ulcer | Defect in epidermis and dermis due to loss of tissue | Pyoderma gangrenosum (Figure 2-13) |
| Eschar | Black, hard crust resulting from tissue necrosis of the epidermis and/or dermis | Self-induced injury (Figure 2-14) |
| Atrophy | Depression and/or surface change in skin as the result of diminution of a component(s) of the epidermis, dermis, or fat | Lichen sclerosis (Figure 2-15) |
| Scar | Depressed or elevated proliferation of connective tissue that has replaced inflamed or traumatized skin | Depressed scar (Figure 2-16) Hypertrophic scar (Figure 2-17) |
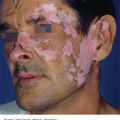
Figure 2-8.
Scale. Psoriasis.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


