Molluscum Contagiosum
Sumul A. Gandhi
David C. Reid
I. BACKGROUND
Molluscum contagiosum (MC) is a common, self-limited viral lesion caused by four closely related subtypes of a DNA-containing poxvirus. Infection occurs worldwide, with viral subtypes varying geographically. In the United States, molluscum contagiosum virus subtype 1 (MCV-1) accounts for 90% of all cases. In the setting of HIV, however, MCV-2 is implicated in approximately 60% of infections.
Viral infection is contracted through skin-to-skin contact, fomite transmission, and autoinoculation. Once exposed, MCV replicates in the cytoplasm of infected keratinocytes. Viral particles may be seen in all epidermal layers, although replication is postulated to occur in the more differentiated cell layers. MCV contains many novel genes, including the IL-18-binding protein gene, that are effective in blocking host immune defenses and enabling viral particle survival and spread.
MCV peak incidence is among children younger than 5 years of age, with a reported lifetime prevalence of up to 25% in some studies. Widespread MC can occur in patients with atopic dermatitis, leukemia, sarcoidosis, and immunosuppressed states, like AIDS.
II. CLINICAL PRESENTATION
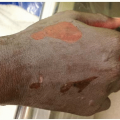
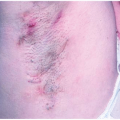
MC lesions are discrete, skin-colored or pearly white, raised, waxy-appearing firm papules 1 to 5 mm in diameter with a central punctate umbilication (Fig. 30-1). MC most commonly occurs on the trunk, thighs, and skin folds. Involvement of the palms and soles is rare. Sexually transmitted MC involves the lower abdomen, groin, genitals, and proximal thigh areas. Widespread, disfiguring lesions can be seen in the setting of immune compromise, as in AIDS. Especially in children with MC in the setting of atopic dermatitis, skin irritation with erythema, scale, and pruritus around MC lesions is common and signifies the development of a host immune response to the virus (Fig. 30-2).
III. WORKUP
Diagnosis is generally made by clinical assessment. However, when necessary, etiology may be confirmed with microscopic or histopathologic examination. A lesion can be incised, smeared between two glass slides, and stained (with Wright, Giemsa, or Gram stain). Using this in-office technique, or obtaining tissue biopsy for hematoxylin and eosin preparation, light microscopy demonstrates keratinocytes that contain eosinophilic cytoplasmic inclusion bodies also known as Henderson-Patterson or molluscum bodies. These inclusion bodies, consisting of virions in various stages of development, push the host cell to the periphery, giving the appearance of a signet ring cell.
In children with MC, no routine laboratory studies are indicated. However, sexually active adolescents and adults with MC should be screened for the
presence of other coexisting sexually transmitted diseases, including HIV, and other sources of immune compromise.
presence of other coexisting sexually transmitted diseases, including HIV, and other sources of immune compromise.
 Figure 30-1. Molluscum contagiosum. Dome-shaped, pink papules with central umbilication. (From Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
 Figure 30-2. Molluscum contagiosum. Characteristic lesions, many excoriated, in the setting of atopic dermatitis of the flexural creases. (From Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


