Mohs micrographic surgery is a specialized form of skin cancer surgery in which the Mohs surgeon acts as both surgeon and pathologist. The procedure is characterized by its histopathologic margin control and ability to spare tissue, particularly in cosmetically sensitive locations. Mohs surgery is known for both limiting the size of the final defect and its high cure rate. In this review, the authors highlight indications for the procedure, detail the technique itself, discuss cutaneous tumors for which Mohs micrographic surgery is indicated, and present the economic benefit of Mohs surgery.
Key points
- •
The practice of Mohs surgery has become increasingly widespread among the dermatologic surgery community and is now considered the treatment of choice for many common and uncommon cutaneous neoplasms.
- •
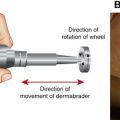
In Mohs surgery, the blade is oriented at a 45° angle to the skin, which is referred to as beveling. Beveling of the scalpel blade allows for proper alignment of the peripheral edges and examination of nearly 100% of the specimen margins.
- •
National guidelines, or “appropriate use criteria (AUC),” were created for Mohs surgery in 2012 based on the characteristics of an individual tumor, anatomic location, and unique patient characteristics.
- •
In general, locally aggressive tumors, tumors arising in locations that necessitate tissue sparing, and patients at highest risk of aggressive tumor abnormality or recurrence are ideal candidates for Mohs surgery.
- •
Mohs surgery is highly effective for most nonmelanoma skin cancers, is cost-effective, and has become the standard of care for many cutaneous tumors.
Introduction
Mohs micrographic surgery (MMS) is a specialized form of skin cancer surgery in which cure rates close to 100% are achieved with minimal tissue removal. The procedure was pioneered by Dr Frederic E. Mohs in the 1930s. In the late 1960s, Dr Mohs, along with Dr Theodore Tromovitch, introduced the fresh-frozen tissue technique used today.
The method of MMS is unique in that the Mohs surgeon acts as both surgeon and pathologist. In most cases, the tumor is removed, histopathology is interpreted, and the defect is repaired, all in the same day. Since Dr Mohs’ initial work in the 1930s, the practice of Mohs surgery has become increasingly widespread among the dermatologic surgery community and is now considered the treatment of choice for many common and uncommon cutaneous neoplasms.
Introduction
Mohs micrographic surgery (MMS) is a specialized form of skin cancer surgery in which cure rates close to 100% are achieved with minimal tissue removal. The procedure was pioneered by Dr Frederic E. Mohs in the 1930s. In the late 1960s, Dr Mohs, along with Dr Theodore Tromovitch, introduced the fresh-frozen tissue technique used today.
The method of MMS is unique in that the Mohs surgeon acts as both surgeon and pathologist. In most cases, the tumor is removed, histopathology is interpreted, and the defect is repaired, all in the same day. Since Dr Mohs’ initial work in the 1930s, the practice of Mohs surgery has become increasingly widespread among the dermatologic surgery community and is now considered the treatment of choice for many common and uncommon cutaneous neoplasms.
History
Dr Frederic E. Mohs devised the technique of Mohs surgery during his time as a medical student. Although working as a cancer research assistant, he found that application of a zinc chloride solution to cancer tissue in vitro led to tumor necrosis with maintenance of tumor histopathology, as if the tissue had been preserved in formalin. He extrapolated this finding to in vivo skin cancers. In his initial experiments, a 20% zinc chloride solution was applied to a skin cancer, allowed to fix overnight, and then the lesion was excised with narrow margins the next day. The specimen was prepared in slides via paraffin embedding and evaluated with light microscopy. If tumor cells were noted at the margin of the specimen, this process was repeated until margins were clear. Because of extensive wound bed damage caused by the zinc chloride solution, the only option for repair after tumor extirpation was healing by secondary intention. Although this led to surprisingly pleasing cosmetic results, the healing process was lengthy, and the procedure itself quite painful for patients. Although Dr Mohs started his work in what he coined “chemosurgery” in the 1930s, his findings were not published until 1941. He continued to modify his method, and in 1953, he performed the first “fresh frozen section,” which is the technique used today.
Dr Mohs discovered the benefits of fresh-frozen sectioning quite by mistake. While filming an educational video about chemosurgery in the 1960s, he was forced to complete the procedure in 1 day. Unable to allow his fixative to sit overnight, he removed an eyelid tumor using local anesthesia and prepared his slides using fresh-frozen sectioning. He found this technique caused less destruction to surrounding normal tissue, and he maintained his impressive 100% 5-year cure rate. Mohs presented his data, a cohort of 70 basal cell carcinomas (BCCs) on the eyelid removed with the fresh-frozen technique, in 1969. The following year, Dr Theodore Tromovitch published a series of an additional 75 cases successfully treated with the fresh-frozen technique. These findings further validated the efficacy of this method.
The fresh-frozen tissue technique quickly became the standard of care, and in 1987, the American College of Chemosurgery was renamed the American College of Mohs Surgery and Cutaneous Oncology to reflect this practice. Despite numerous changes to the original method, MMS remains one of the few methods of treating cutaneous malignancies with a cure rate nearing 100%.
Mohs micrographic surgery: preoperative considerations
MMS is typically performed as an outpatient procedure under local anesthesia in a dermatology office. As with any surgical procedure, a careful review of the medical record is performed. Specific considerations include antibiotic prophylaxis in compliance with the American Heart Association (AHA), American Academy of Orthopedics, and American Dental Association guidelines, careful review of implantable devices (as electrodessication devices may cause interference), verification of prescription or nonprescription anticoagulants, HIV and hepatitis C status, allergies, and oxygen requirements.
Antibiotic Prophylaxis
In 2007, the AHA published revised guidelines on the use of antibiotics for endocarditis prophylaxis before minor procedures. Their current recommendations indicate that endocarditis prophylaxis is only necessary in cases involving infected skin or in patients with prosthetic implants, a history of endocarditis, cardiac valve disease after cardiac transplant, or history of cyanotic congenital heart disease. In addition, prophylaxis may be given to patients who have received an orthopedic implant in the 2 years before their procedure or any patient with a history of a previously infected joint.
For patients requiring antibiotic prophylaxis, the AHA recommends 2 g amoxicillin administered by mouth 30 to 60 minutes before their procedure, because it allows antibiotics to be in the bloodstream at the time of incision and in the wound coagulum at the time of procedure completion. Alternative antibiotic choices include cephalexin 2 g by mouth or, for penicillin-allergic patients, clindamycin 600 mg by mouth. If the preprocedure antibiotic dose was missed inadvertently, the medication may be given up to 2 hours after the procedure.
Anticoagulants
In the authors’ practice, they recommend patients continue their anticoagulant medications during MMS because most cutaneous and subcutaneous bleeding is easily managed with electrodessication. For patients receiving warfarin, a prothrombin time and international normalized ratio are obtained 1 week preoperatively. Surgery should be avoided in patients with supratherapeutic anticoagulation.
Implantable Devices
The use of electrodessication to achieve hemostasis is of particular concern in patients with a pacemaker and/or defibrillator as well as other implanted electrical devices, including deep brain stimulators and pain pumps. Traditionally, the use of electric current is contraindicated in these patients because of risk of device malfunction from electromagnetic interference. Device destruction, reprogramming, or battery depletion may also occur. More recent in vitro studies indicate that electrodessication with a hyfrecator on maximal settings may be used safely beyond a 3-cm radius around the implanted device or beyond a 1-cm radius with standard settings. Use of short, 1-second bursts of electricity, as opposed to longer bursts, further improves the safety of hyfrecator use in the setting of implanted devices. In oxygen-dependent patients, oxygen flow is temporarily discontinued while using electrical means of hemostasis because the spark could ignite a fire.
Mohs micrographic surgery: surgical technique
MMS is customarily performed in a nonsterile, minor procedure room. Studies have shown that clean, nonsterile gloves are safe and effective for this procedure without altering infection rates during tumor extirpation. In fact, a recent systematic review and large meta-analysis showed that no difference was found in the rate of postoperative surgical site infections between outpatient surgical procedures performed with sterile versus nonsterile gloves.
Obtaining informed consent before MMS is unique and nuanced in comparison to other dermatologic procedures. The final defect size and subsequent repair are estimated before the procedure. There exists a high likelihood that the tumor may extend beyond what is evident to the naked eye, referred to as subclinical extension. Factors associated with subclinical extension include tumors greater than 1 cm in diameter, recurrent tumors, and tumors with fibrosis noted on initial biopsy. It is essential to discuss expectations of final defect sizes and potential repair options with the patient.
Once informed consent is obtained, the biopsy site is identified. In an effort to avoid wrong site surgery, biopsy site confirmation is of the utmost importance. This identification, however, can present a challenge. Small biopsy specimens are frequently sampled, resulting in a small wound or scar. Lag time between the biopsy and surgery in addition to background actinic damage compounds the issue. Furthermore, patient confusion can play a role as they may have had multiple procedures (on separate tumors) scheduled on the same day. Since the exact site is not always readily visible, patients can point to the precise biopsy site with a cotton tip applicator while holding a hand-held mirror. Multiple studies have shown, though, that the patient may identify the incorrect site of the biopsy. One such study revealed that 16.6% of patients and 5.9% of physicians incorrectly identify biopsy sites. When preoperative photographs were available in this study, the correct site was always identified. As such, photography at the time of biopsy is perhaps the best way to ensure that the biopsy site is evident at the time of surgery.
Several additional strategies may be used to aid in the identification of the correct site. Rubbing the site with cotton gauze produces hyperemia and/or superficial abrasions in the biopsy site. In addition, visualization of the area with a dermatoscope can assist in revealing residual tumor or scar tissue. A patient may argue that if the tumor is not clinically visible, there is no need to proceed with surgery. However, although residual tumor was clinically observed in only 12% of patients, histologically apparent tumor was present in 69% of cases.
Procedure Preparation
Once the site is confirmed, the patient is placed in a recumbent position, and the area is cleansed with an antiseptic, such as chlorhexidine. Before injecting local anesthesia, a surgical ink pen is used to delineate clinically evident tumor or boundaries of the biopsy scar. Marking the site before injection of local anesthesia is preferred because the fluid’s tumescence distorts the site and obscures clear delineation of the scar/tumor margins.
Once anesthetized, a reusable curette is used to gently scrape the tumor. Curettage debulks the tumor to allow for proper fixation of the peripheral edges of the specimen by the histotechnicians. Bulky, thick specimens are more technically challenging to process. In addition, data have shown that the use of curettage reduces the number of stages needed to clear the tumor, because it helps to delineate the margins of the tumor.
Following curettage, a 1-mm (mm) peripheral margin is marked with the surgical ink pen. Reference marks are placed at the 12, 3, 6, and 9 o’clock positions to ensure precise orientation ( Fig. 1 ). Some surgeons choose to create superficial nicks or reference marks with the blade versus the surgical ink pen. All methodologies for specimen marking are to properly orient the specimen and allow anatomic triangulation of any residual tumor based on histopathologic interpretation.

Excision of the First Layer
In most cutaneous excisions, the blade is oriented at a 90° angle to the skin in order to more closely approximate the skin during repair. In MMS, the blade is oriented at a 45° angle to the skin, which is referred to as beveling ( Fig. 2 ). Beveling of the scalpel blade allows for proper alignment of the peripheral edges of the tissue specimen during preparation of the histologic specimen.

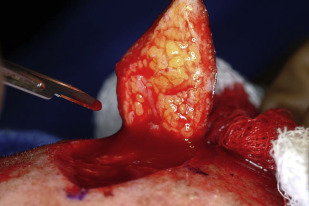
Once the Mohs surgeon scores the skin in a beveled fashion, the tumor is excised with careful attention to remove a thin specimen in a flat, horizontal plane immediately below the depth of previous curettage ( Fig. 3 ). Obtaining a flat, disc-shaped specimen is imperative, because it helps ensure proper processing of the specimen onto slides in a horizontal plane. Hemostasis is obtained with electrodessication, and the patient is temporarily bandaged. During slide preparation and evaluation, the patient is free to wait in a comfortable waiting area.
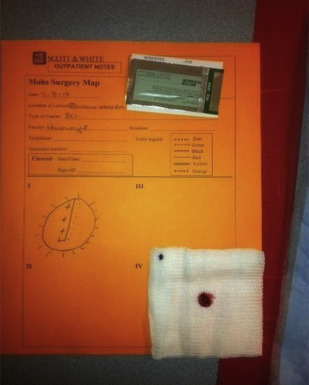
The tissue is placed on surgical gauze with careful attention to maintain the anatomic orientation of the specimen. The tissue is transported to the histology laboratory, where the MMS map is produced ( Fig. 4 ). The map is an essential tool that correlates the surgical site, tissue specimen, and histologic slides produced. Extreme care is taken to maintain precise orientation of the specimen and map, because the map serves to guide future stages of tumor removal should the margins be involved in the first or subsequent stages.
Processing of the Surgical Specimen
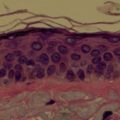
The first stage is inked and mapped with a drawn representation on the Mohs map ( Fig. 5 ). The inked tissue is cut into appropriately sized blocks to fit onto a glass slide. The specimen is flattened, often by using relaxing shallow cuts parallel to the epidermal edge, in order for the epidermis to lie evenly in the same plane as the deep margin. This step is crucial and allows the epidermis and the subcutaneous fat to both be visualized by the Mohs surgeon on the glass slide with the goal of examining 100% of the specimen’s margin.