Chapter 51 Milagro (Beta-Tricalcium Phosphate, Polylactide Co-Glycolide Biocomposite) Interference Screw for Anterior Cruciate Ligament Reconstruction
Introduction
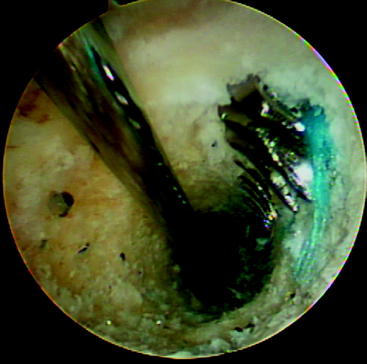
The initial interference fixation screws were made from metal and provided screw fixation for anterior cruciate ligament (ACL) reconstructions. Biodegradable interference fixation screws subsequently gained wide acceptance after their introduction in the early 1990s.1–5 The benefits of these biodegradable interference screws include reduction in the concerns previously associated with metal implants, including difficulties in postoperative imaging, reduced graft laceration during insertion, less chance of screw divergence during insertion, easier revision surgery (Fig. 51-1), and fewer problems with secondary arthritic procedures that might require the complete removal of a metal screw. In addition, the load to failure (LTF) strength of these screws is sufficient to allow for an aggressive rehabilitation program. Potential complications associated with biodegradable interference screws include the risk of screw breakage during insertion, decreased holding strength when compared with a metal alternative, and inflammatory reactions that could lead to lytic changes and cyst formation.
Poly-L-lactic acid (PLLA) is the most common material used in biodegradable interference screws. These screws offer effective graft fixation with little evidence of adverse inflammatory reactions, and many years pass before any material degradation occurs.1–8 Interference screws made of lactic acid copolymers containing dextro and levo stereoisomers subsequently became available, as did copolymers of polylactic acid and polyglycolide. The polymer degradation is more rapid with poly D, L-lactide (PDLLA) implants than pure PLLA in animal studies.9–11
Biomechanical and Biochemical Data
Implant degradation proceeds through five stages: hydration, depolymerization, loss of mass integrity, absorption, and elimination. How rapidly an implant is degraded is influenced by the polymer of which the implant is made, the degree of crystallization of that polymer, the initial mass of the polymer present (implant size), surface coverings, whether the polymer is self-reinforced, the processing technique used (machining or injection molding and sterilization technique), and the environment in which the implant is situated.12 In addition, the degradation mechanics of different polymers may differ considerably based on the hydrophilic or hydrophobic nature of the different polymers.
Degradation starts at the amorphous phase of the implant and leads to fragmentation of the material to smaller parts, which are then phagocytosed primarily by macrophages and polymorphonuclear leukocytes.13,14 The lactic acid component is broken down by hydrolysis. The resultant monomers enter the Krebs cycle and are further dissimilated into carbon dioxide and water.15 In addition to hydrolytic chain scission, glycolic acid monomers are degraded by the enzymatic activity of esterases and carboxypeptidases.16
All biodegradable materials cause some inflammatory response. The longer the degradation course, the less visible the response will be. Usually there is a mild, nonspecific tissue response with fibroblast activation and the invasion of macrophages, multinucleated foreign body giant cells, and polymorphonuclear leukocytes during the final stages of degradation. Because of the more rapid degradation associated with polyglycolic acid (PGA), there have been some foreign body reactions with varying degrees of severity ranging from mild osteolytic changes to intense granulomatous inflammatory soft tissue lesions that necessitate surgical intervention.17,18
Concerns about implants composed of pure PGA have led to the development of PGA copolymers that still have a more rapid rate of absorption compared with PLLA implants, but the literature supports their use with excellent clinical results. Lajtai et al19,20 reported good results with a lactide/glycolide copolymer screw (85/15, D, L lactide/glycolide). Using magnetic resonance imaging (MRI scans), the screw was shown to remain intact for 4 months and then disappear by 6 months. Five years after implantation, the screw was completely reabsorbed and evidently replaced with new bone. Morgan et al21 evaluated a PLLA interference screw removed en bloc from a patient 2.5 years after insertion. The histological examination and molecular weight measurements showed a 75% decrease in the molecular weight of the screw with implant fragmentation and new bone formation adjacent to the screw. This dramatically contrasted with the MRI evaluation of the patient, which showed the presence of a clear screw outline. MRI evaluations of PLLA screw show no evidence of any progressive absorption 4 years after implantation.22 However, a recent computed tomography (CT) evaluation of patients who underwent patellar tendon autograft ACL reconstruction using PLLA screws at least 7 years earlier demonstrated complete removal of the PLLA screws without any significant bone ingrowth into the screw site.23
Basic Science of Beta-Tricalcium Phosphate copolymers
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


