Key points
- •
Adequate markings on the skin.
- •
Suitable skin dissection.
- •
SMAS/platysma flap elevation.
- •
Midface treatment.
- •
Skin sutures.
Patient selection
The decision as to whether to perform a rhytidoplasty on a person must be preceded by the patient’s request for the surgery and preparation for the procedure. The surgeon must know precisely what the patient wants and what their expectations are. When you feel the patient is suitable for the operation you can then thoroughly examine the face, assessing the skin quality, the bony skeleton, the deformities and magnitude of the alterations and the potential difficulties such as retraction of the mandible, bad position of the hyoid bone, fat amount, skin elasticity, lack of skin elasticity, etc. Facial asymmetry should be shown and discussed with the patient prior to surgery so that after the operation, an unobserved unilateral deformity not noticed by the patient beforehand does not create a problem post-operatively. Surgical limitations and your own limitations should also be explained to each patient.
During the consultation period, it is important to understand what the patient’s expectations are so that the operation is performed for the patient and not for the surgeon. Occasionally, a major extensive procedure is performed, increasing the risks of a complication, just to eliminate or alleviate a deformity the patient has never noticed in order to satisfy a surgeon’s ego. One must be aware that the results are not the same. A patient who has surgery for facial rejuvenation in their sixties or seventies will never have the same result as a patient who undergoes a facelift in their forties or fifties and an attractive patient will attain a better result than one who is less attractive. Time causes beauty to fade so procedures for rejuvenation performed on a good candidate will increase beauty, whereas the same procedures performed on a unattractive one may not. A patient with an oval shaped face will likely have a better aesthetic result than a patient with a round one.
Indications
Rhytidoplasty is recommended for patients who are not happy with their facial appearance due to the natural aging process. The reasons for surgery must be carefully assessed and clearly understood by the surgeon as the decision to undergo surgery is not taken overnight and it is likely that the patient will have been considering the prospect for a long time. When a patient encounters someone who has already undergone this procedure they may be enthusiastic and quickly consult a plastic surgeon. However, their expectation may be much higher than the reality of the outcome and for this reason they are not the ideal patient.
Alterations on the face desired by the patient are evaluated in detail and discussed, so that the result we hope to obtain in that particular patient can be previewed. Skin quality such as elasticity and hydration is noted. The location of sideburns, the distance between the hairline and lateral canthus and the appearance of the tragus are very important in determining the perfect location of the incisions. Alterations on the ear contour and dislocation of sideburns may cause signs that denote surgery was performed. Photos in front and profile view are taken. This documentation is useful during the surgery and also to judge the result. Besides front and profile positions, close up of the eyelids, ear contour and patient facing downwards may also be helpful. Patients must be in perfect physical and psychological health to undergo facial rejuvenation surgery. Blood tests, urine analysis, heart exams, lung X-rays and a consultation with a GP are required. Medications that the patient is taking are also discussed and noted.
Operative technique
Pre-operative preparation
The patient goes to the hospital on the day of the procedure. An assistant then prepares the hair for the incisions according to where the incisions will be made, and the anesthesiologist decides the type of anesthesia best suited for the particular patient. The patient will then proceed to the operating room and is operated on under local with sedation or general anesthesia. Skin markings are made and then an infiltration of 0.5% lidocaine with epinephrine 1 : 200 000 is performed (approximately 80 cc for each side).
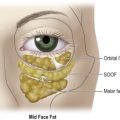
The areas to be undermined and the incisions to be made on the SMAS are marked on the skin with methylene blue. Where the midface is to be elevated, we mark the ideal point for the suture ( Figure 10.1C ). The surgery usually starts with an incision behind or in front of the ear where there will be a short scar. In the pre-auricular area usually I do a pre-tragal incision which goes into the hair to the temporal area or follows the sideburns. A combined incision in the temporal area and contouring the sideburns is also common. The retroauricular incision stops at the ear lobe or ascends following the retroauricular sulcus entering at the hairline. Commonly, skin undermining is ample and in most cases, connects the face in the submental area.

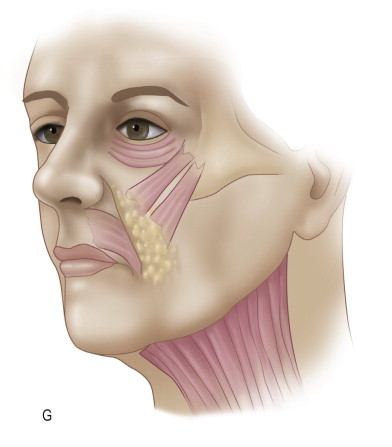
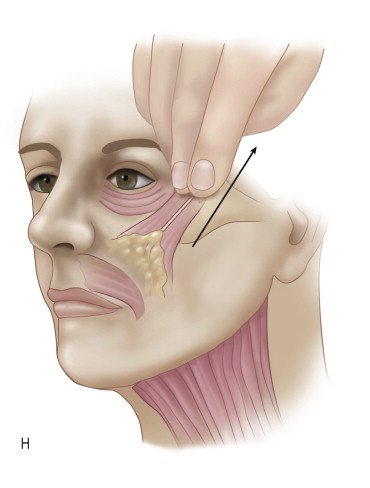
After skin undermining and hemostasis is complete, an extended incision over the zygoma is marked. This incision goes towards the previously marked point over the malar zone ( Figure 10.2 ). An incision on the SMAS in front of the ear is then made. This incision goes inferiorly passing approximately 1 cm behind the mandibular angle (in order to avoid injury to the mandibular branch of the facial nerve) and descends approximately 6 cm below the lower extremity of the mandible. The SMAS–platysma flap is then elevated. Normally I start the dissection in the upper portion (zygoma) descending to the platysma. My preference is to dissect the SMAS–platysma using the scalpel, but this is a personal choice. It can also be performed using scissors or the Colorado tip electrocautery. During this dissection the flap is pulled posteriorly so that I can calculate the correct tension to be applied to the tissues.
When I decide the traction is sufficient to obtain the desired effect, the flap is pulled in a superior and posterior direction, and sutured to the aponeurosis of the temporal muscle or any fixed structure such as the periosteum of the zygoma. The most anterior portion of the superior flap is then pulled superiorly and obliquely and sutured to the periosteum of the malar bone in order to elevate and reposition the tissues of the midface ( Figure 10.3 ). The central portion of the flap is pulled in a superior direction and sutured to the zygoma. The flap in front of the ear is severed superiorly, but left attached inferiorly and rotated to a position behind the ear to give a better definition of the lower border of the mandible. This flap is sutured into a fixed anatomic point behind the ear.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


