Introduction
The middle or central skull base has customarily been delineated from the anterior skull base by a horizontal line along the anterior sellar margin (tuberculum sellae), which extends laterally along the posterior margin of the lesser wing of the sphenoid bone on both sides and includes the medial anterior clinoid processes. The posterior boundary of the middle skull base is formed medially by the dorsum sella and laterally by the petrous ridges. The appearance of the skull base, as viewed from above and through an open calvaria, naturally separates the skull into its three classic anatomical divisions. The anatomical boundaries of the skull base coincide with the boundaries of the proposed intracranial spaces, producing the anterior, middle, and posterior cranial fossae. This archetypical approach does not take into account the practically important, three-dimensional (3D) connections of the middle skull base in the current era of advanced cross-sectional imaging or the availability of sophisticated surgical and radiation treatment methods.1,2
The 3D anatomy of the middle skull base should encompass the contiguous anatomical regions of the orbital apex and optic canal, including the optic nerve leading posteriorly to the optic chiasm, the superior orbital fissure, the pterygopalatine fossa, and the sella. In addition, the suprasellar and parasellar structures, including the pituitary gland and stalk, cavernous sinus, internal carotid artery, cranial nerves, Meckel’s cave, regional skull-base foramina, sphenoid sinus, clivus, petrous apex, petro-occipital fissure, foramen lacerum, and parts of the nasopharynx should also be incorporated as part of the middle skull base. This region can be conceptualized as having a roughly spherical shape with the optic chiasm at the superior pole, nasopharynx at the inferior pole, pterygopalatine fossa at the anterior pole, and the foramen ovale at the lateral and prepontine cistern at the posterior poles, respectively. Attributing a 3D configuration to the middle skull base allows for compartmentalization of the anatomy, which in turn helps to predict pathology based on the knowledge of intrinsic structures dwelling in the particular location. In addition, it sheds light on the complex anatomical connections and aids in assessing the origin and spread of various transspatial disease processes. The lateral aspect of the middle skull base, constituted predominantly by the greater wing of the sphenoid bone, forms the floor of the middle cranial fossa, which houses the temporal lobes of the brain.1,3
Center of the Sphere: Sphenoid Bone and Sphenoid Sinus
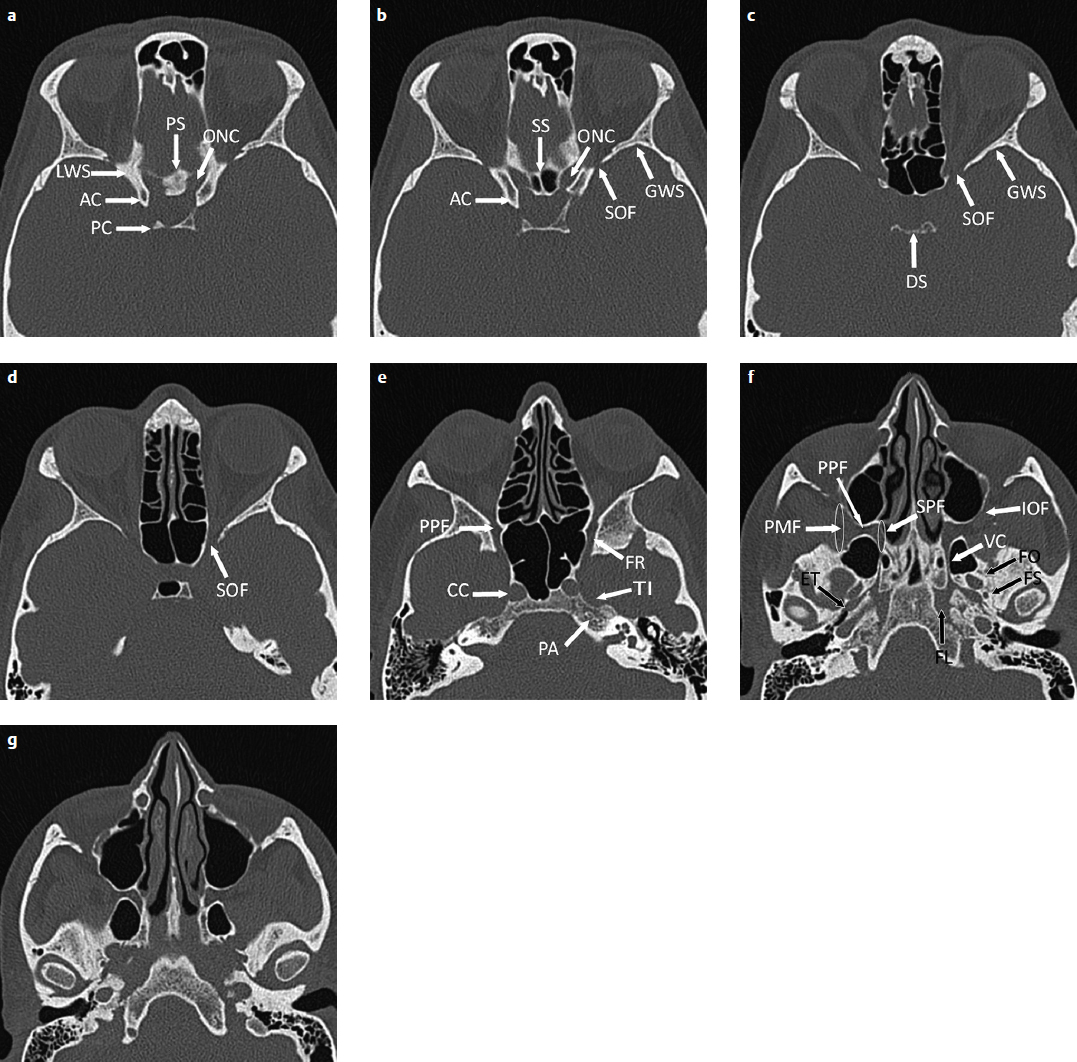
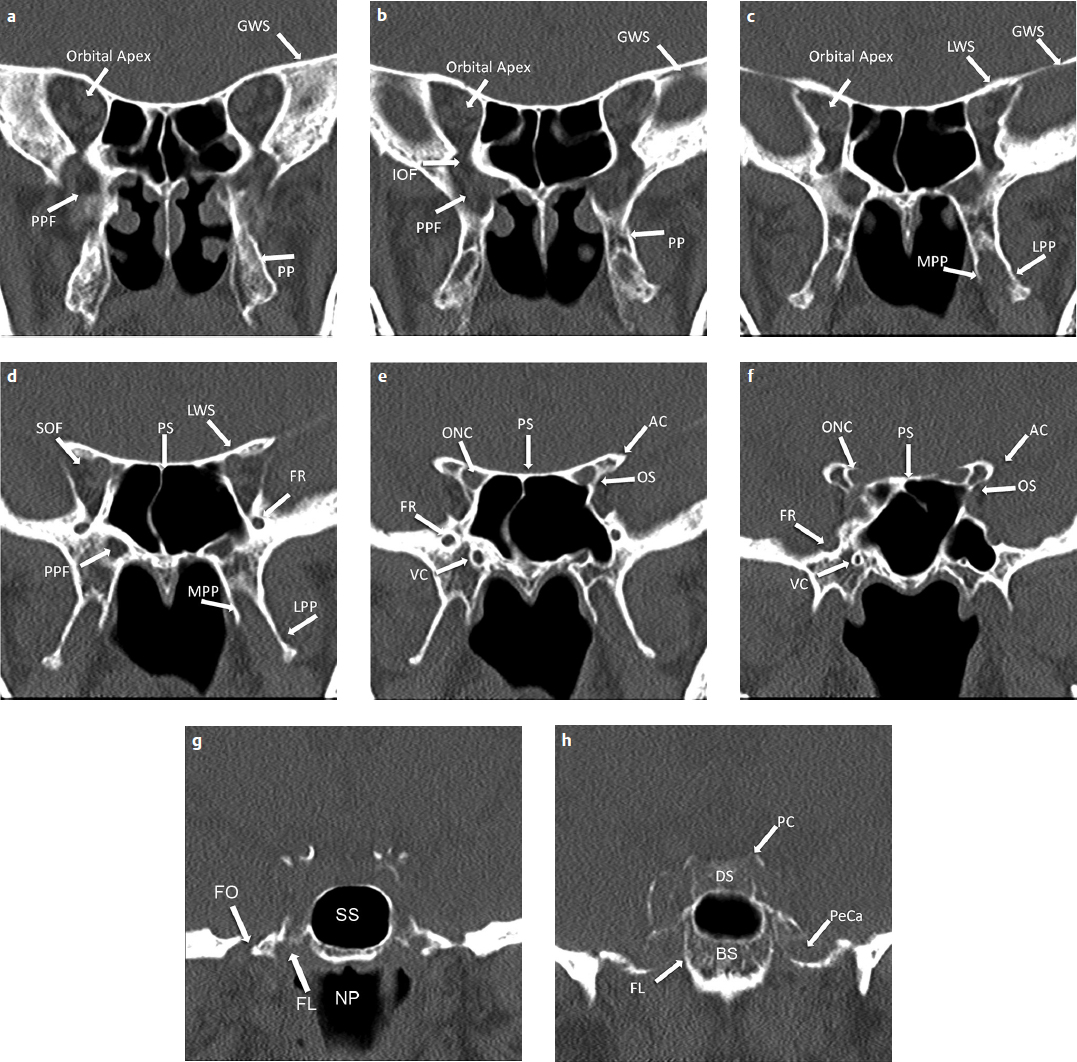
The sphenoid bone has a central body and is constituted on either side by the lateral greater and lesser wings and the inferior pterygoid process with the medial and lateral pterygoid plates. The body of the sphenoid contains the sella turcica superiorly and the sphenoid sinus inferiorly. Posteriorly, it forms the anterosuperior aspect of the clivus, joining the posteroinferior aspect from occipital bone at the spheno-occipital synchondrosis. The spheno-occipital synchondrosis separates the basisphenoid from the basiocciput (Fig. 3.1). Chordomas can arise from notochordal remnants near the synchondrosis, and the presence of vascularized bone marrow predisposes the clivus to pathologies like myeloma and metastasis. The lesser wing of the sphenoid forms the posterior margin of the anterior skull base—harboring the optic canal. The greater wing of sphenoid forms the floor of middle cranial fossa. The superior orbital fissure lies between the lesser wing of the sphenoid superomedially and the greater wing of the sphenoid inferolaterally, separated by the optic strut, a small bony bridge that projects from the anterior clinoid process of the lesser wing to the sphenoid body.4,5 The osseous architecture of the sphenoid bone, sphenoid sinus, and associated relationships with adjacent osseous skull base, canals, and foramina is best studied with high-resolution computed tomography (CT) scans using thin slices and bone algorithms (Fig. 3.2, Fig. 3.3).
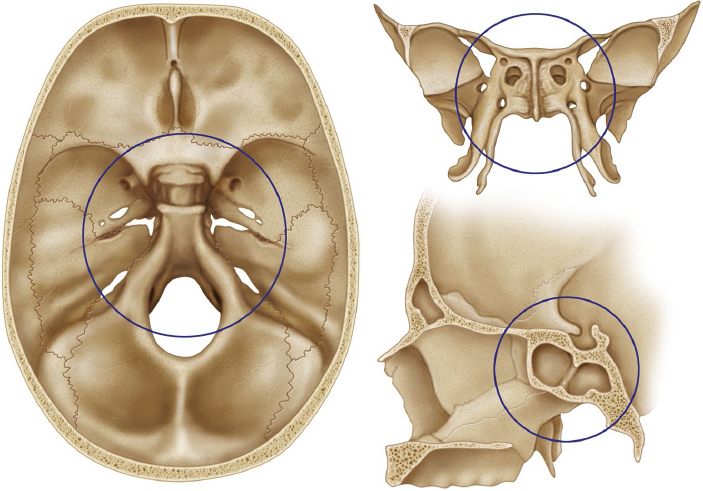
Fig. 3.1 Three-dimensional illustrations of the superior, anterior, and lateral views of the sphenoid bone and the osseous foundation of the central skull base. The outlined spherical region denotes the central skull base region and includes the adjacent endocranial structures including the pituitary gland and the exocranial structures of the neck including the nasopharynx.
The extent of sphenoid sinus pneumatization (or lack thereof) is classified as conchal, presellar, and sellar.6 In the conchal form, the sphenoid bone is essentially solid without development of an aerated sphenoid sinus. With presellar pneumatization, the sphenoid sinus is pneumatized but does not extend posteriorly to the coronal level of the anterior sellar. With sellar pneumatization, the sphenoid sinus extends posteriorly inferior to the sella and can extend to the posterior clival margin. The anterior wall and floor of sella are quite thin in the latter subtype, measuring less than a millimeter in thickness. Sphenoid sinus pneumatization may extend into the optic strut and anterior clinoid process, resulting in thinning of the boundary with the optic canal and superior orbital fissure. Passage of the vidian canal through the body of sphenoid bone and the foramen rotundum, along the lateral aspect of sphenoid sinus roof, lies in close relation to sphenoid sinus.7 The sphenoid sinus lies close to the internal carotid arteries (ICAs) and cavernous sinuses. The ICA lies along a shallow groove on the intracranial side of the lateral wall of the sphenoid sinus. The variable intercarotid distance between the ICAs of both sides makes pituitary surgery more risky. Sphenoid sinus septation also varies considerably. Although it is usually single, septation can be multiple with septa deviating laterally, inserting near the carotid artery.8 Contiguous spread of pathology, bony destruction, and potential for iatrogenic injury to adjacent critical structures during surgery should be carefully estimated during presurgical imaging evaluation of the sphenoid sinus.
Intracranial Structures Superior to Center of the Sphere
Sella Turcica and Suprasellar Region
The sella turcica (Turkish saddle) is a saddle-shaped depression in the body of the sphenoid bone. The seat of the saddle supports the pituitary gland and is known as the hypophyseal fossa (Fig. 3.4). Its anterior margin is the tuberculum sella, and its posterior margin is the dorsum sella, with the superolateral posterior clinoid processes on either side. The dorsum sella is continuous posteriorly with the clivus. The chiasmatic sulcus lies just anterior to the tuberculum sella and medial to optic canals. The planum sphenoidale, a part of the anterior cranial fossa, lies in front of the tuberculum sellae and chiasmatic sulcus. The medial processes along lesser wings of sphenoid bilaterally form the sella’s anterior clinoid processes. The floor of the pituitary fossa has a well corticated, less than 1-mm-thick bony wall known as the lamina dura. The diaphragma sellae is a slightly inferior, convex, thin dual fold covering the superior aspect of sella and is perforated centrally by the pituitary stalk. The pituitary stalk passes through the cerebrospinal fluid (CSF) filled suprasellar cistern on its way to the hypothalamus. The suprasellar cistern also houses the optic chiasm and circle of Willis. Large sellar or suprasellar lesions, including pituitary adenomas and craniopharyngiomas, can produce optic chiasm compression.
Cavernous Sinus
The cavernous sinuses, dural venous sinuses lying on either side of the sella connected by intercavernous sinuses, are fed by multiple tributaries, including the superior ophthalmic veins in the orbits, sphenoparietal sinuses seen along the anterior aspect of middle cranial fossa, basal vein of Rosenthal seen in the perimesencephalic cisterns draining toward the vein of Galen, pterygoid venous plexus seen in the masticator space, and the basilar venous plexus near the petrous apex. They drain through the superior petrosal sinus into the sigmoid sinus and through the inferior petrosal sinus into the internal jugular vein. In a carotid-cavernous fistula, venous channels may be engorged with high pressure arterialized flow and appear enlarged on magnetic resonance imaging (MRI) and CT scan images.9
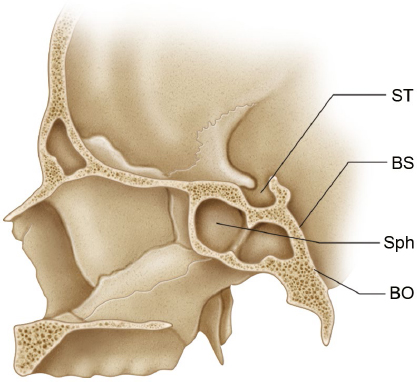
Fig. 3.4 Sagittal illustration through the central skull base demonstrates the bony anatomy of the sella trurcica (ST). The anterior wall of the sella is very thin and separates the sella from the sphenoid sinus (Sph). The clivus is formed by the basisphenoid (BS) superiorly and the basiocciput (BO) inferiorly.
The cavernous sinus has five walls.1,10 The medial wall of the cavernous sinus consists of an upper sellar component with a single-layered, thin, dural membrane separating it from the lateral margin of the pituitary gland, and a lower, thicker component adherent to the carotid sulcus. Tumor obliteration of the medial venous compartment of the cavernous sinus inferior to the cavernous ICA in a coronal MRI scan (called carotid sulcus venous compartment of cavernous sinus) has been shown to have a 95% positive predictive value (PPV) for cavernous sinus invasion by a pituitary adenoma.11 Perimeter encasement of 67% or more of the cavernous segment of the ICA (100% PPV) and tumor spread beyond the border joining the lateral wall of the intracavernous and supracavernous ICAs (85% PPV), as seen on coronal MRI, both suggest cavernous sinus invasion. If the percentage of encasement of the perimeter of the intracavernous ICA is less than 25%, or if adenoma invasion does not cross beyond the adjoining medial wall of the intracavernous and supracavernous ICAs, cavernous sinus invasion can then be ruled out with a negative predictive value of 100%.
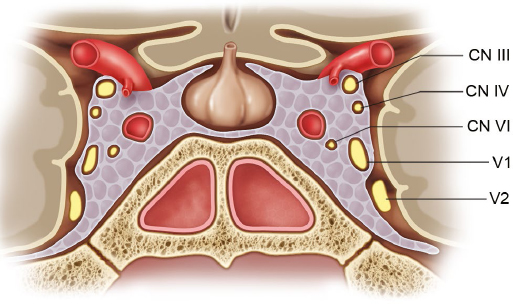
Forming the medial margin of the temporal lobe, the bilaminar lateral wall of the cavernous sinus consists of a thin outer meningeal layer and a thicker inner dural layer that extends from the region of superior orbital fissure and the anterior clinoid process anteriorly to the petrous apex posteriorly. The oculomotor nerve (cranial nerve III, or CN III), the trochlear nerve (CN IV), and the ophthalmic segment of the trigeminal nerve (CN V1) are contained within the lateral wall layers, and the only truly intracavernous nerve, namely, the abducens nerve (CN VI), lies within the cavernous sinus itself, along with the cavernous segment of ICA (Fig. 3.5). Inferiorly, the medial and lateral walls fuse along the lateral margin of the body of sphenoid bone. It is interesting to note that this fusion occurs just superior to the maxillary nerve (second division of the trigeminal nerve, CN V2) and that the CN V2 and mandibular nerve (third division of the trigeminal nerve, CN V3) are not part of the cavernous sinus, even though they are invested by the contiguous dura.1,12
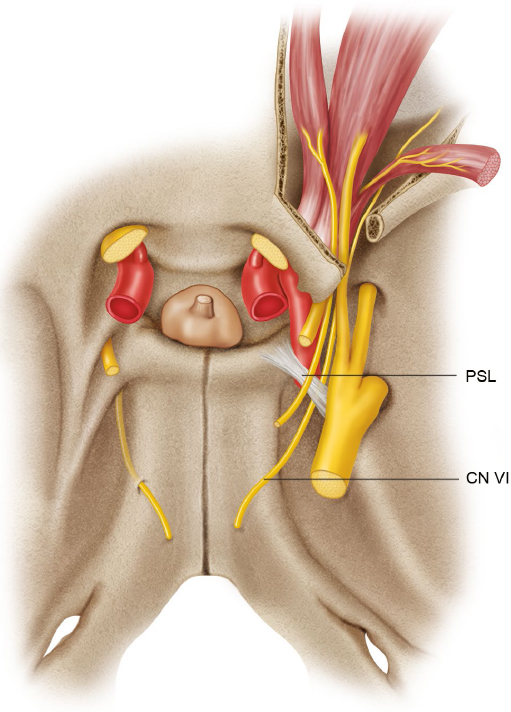
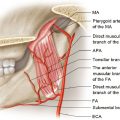
The cavernous sinus becomes contiguous with the inferior petrosal sinus (which in turn drains through the petroclival fissure into internal jugular vein) posteriorly. The posterior wall of the cavernous sinus extends from the lateral margin of the dorsum sella to the superomedial aspect of Meckel’s cave. Just posteroinferior to this is the petrous apex, over which the abducens nerve (CN VI) travels underneath the petrosphenoid ligament, goes through the Dorello’s canal, enters the posterior wall of the cavernous sinus, and is seen within the substance of the cavernous sinus lateral to the cavernous ICA (Fig. 3.6). Petrous apicitis can lead to Gradenigo syndrome with CN VI palsy (resulting from involvement in Dorello’s canal) and trigeminal distribution pain from spread of inflammation into the adjacent Meckel’s cave, where the trigeminal ganglion resides.13
The rectangular anterior wall of the cavernous sinus extends from the optic strut under the anterior clinoid process toward the superior orbital fissure, and its inferior margin forms the superior end of foramen rotundum carrying CN V2. The cavernous sinus roof extends from the optic strut and superior orbital fissure anteriorly to the petrous apex and the edge of the tentorium posteriorly. It is contiguous with the diaphragma sellae medially and is separated laterally from the lateral wall of cavernous sinus by the anterior petroclinoid fold. The anterior petroclinoid fold is a cordlike thickening of the dura extending from the anterior clinoid process anteriorly to tentorial edge posteriorly. The posterior petroclinoid fold is a separate fold extending from the posterior clinoid process to the tentorial edge, whereas the interclinoid fold is a thin band of dura that extends from the anterior clinoid process to the posterior clinoid process. The anatomical importance of these three folds is that they form a landmark triangle at the cavernous sinus roof—the oculomotor triangle (Fig. 3.7). CN III pierces the oculomotor triangle from a posterosuperior aspect to pass through a short oculomotor cistern and enters within the bilaminar lateral wall of the cavernous sinus near the anterior clinoid process. CN IV enters the oculomotor triangle posterolaterally, just posterior to the oculomotor nerve.14
Internal Carotid Artery
The ICAs are important structures that are intimately related to the middle skull base, except for the proximal cervical and distal communicating segments. The widely used Bouthillier system divides the ICA into a seven-segment numerical scale along the superiorly oriented direction of blood flow according to a detailed understanding of the surrounding anatomy and the compartments through which it travels (Fig. 3.8),15 including the following segments from its origin in the neck to its termination at the circle of Willis: cervical (C1), petrous (C2), lacerum (C3), cavernous (C4), clinoid (C5), ophthalmic (C6), and communicating (C7) segments. Cervical C1 segment of the ICA has no branches, enters the carotid canal at the skull base, and travels medially in the carotid canal as the petrous C2 segment, surrounded by bone at its most solid posteromedial and relatively thinner anterolateral and inferior walls, with the roof being covered by dura. The petrous segment of ICA branches are the small caroticotympanic arteries, which enter the middle ear and the occasionally present vidian artery that usually arises from the maxillary artery, which in turn is a branch of the external carotid artery. The petrous carotid artery ends medially partially surrounded by fibrocartilaginous tissue contiguous with the cartilage of the foramen lacerum, over which the ICA passes as the lacerum C3 segment. The foramen lacerum is not within a single bone; rather, it is actually a cartilage-filled gap separating the petrous apex from the basisphenoid medially and the basiocciput posteriorly. Meningeal branches of the ascending pharyngeal artery pass through the cartilage-filled foramen.1 Then the ICA turns superiorly on its way to the cavernous sinus, passing under a fibrous band called the petrolingual ligament (which extends from the petrous apex to the lingula of the carotid sulcus of the sphenoid body), after which the cavernous C4 segment begins. The petroshenoid ligament or Gruber’s ligament (which extends from the petrous apex to posterior clinoid process) is situated superior to the petrolingual ligament, and the abducens nerve (CN VI) lies just lateral and parallel to the horizontal portion of the cavernous ICA underneath the petroshenoid ligament.16–18
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


