Key points
- •
Androgenetic alopecia is a frequent cause of hair loss and hair thinning for both men and women, and it has the potential to negatively affect self-esteem, psychosocial functioning, and quality of life.
- •
Micropigmentation, also known as medical tattooing or dermatography, conveys the aesthetic use of tattooing for medical purposes. ,
- •
Scalp micropigmentation is a cosmetic procedure used as a concealer to address hair loss involving the scalp, and it can be used to lessen the contrast between the hair and skin colors to create the illusion of hair density (level of evidence: 4).
- •
The scalp micropigmentation procedure uses a device with needles to implant metabolically inert pigment granules into the upper and mid-papillary dermis, and it is this level of placement that is the determining factor for the pigment to be retained uniformly.
- •
Scalp micropigmentation can be used as an adjunct to hair transplantation and medical therapies and to cover unwanted scars on the scalp.
Background, definitions, and history
Androgenetic alopecia (AGA) affects millions of men and women around the world. The hair loss or hair thinning that results from AGA may inflict psychological comorbidities and thus diminish quality of life (QoL) (level of evidence: 5). Curative options for AGA are not currently available; however, dermatologists and hair transplant surgeons should discuss all potential treatment modalities to mitigate the effects of AGA. Cosmetic approaches to scalp and hair deformities offer additional therapeutic options to medical and surgical treatments generally used by clinicians. This chapter will focus on scalp micropigmentation (SMP) and microblading as cosmetic camouflaging options for AGA and thinning eyebrows, and the necessary variables to ensure positive outcomes for patients with hair loss.
SMP was first introduced as a safe and effective technique to conceal hair and scalp deformities by Traquina in 2001 (level of evidence: 4). , SMP is a noninvasive procedure that may be used in any type of alopecia regardless of etiology, gender, or extent of hair loss (  ). The technique requires inserting a specialized ink into the upper dermis in a stippling pattern (level of evidence: 4). , The stippling pattern resembles painted dots that mimic hair follicles and aims to visually camouflage any areas of alopecia. The illusion of increased hair density created by SMP reduces the skin-to-hair color contrast. SMP differs from body tattooing in that the anatomy of the scalp differs from that of the skin on the body.
). The technique requires inserting a specialized ink into the upper dermis in a stippling pattern (level of evidence: 4). , The stippling pattern resembles painted dots that mimic hair follicles and aims to visually camouflage any areas of alopecia. The illusion of increased hair density created by SMP reduces the skin-to-hair color contrast. SMP differs from body tattooing in that the anatomy of the scalp differs from that of the skin on the body.
One of the oldest uses of the word “tattoo” is in the Polynesian language. The Polynesians defined tattoos as black pigment placed under the skin. Medical tattooing involves implantation of exogenous, metabolically inert, colorfast pigments into the scalp (SMP) or skin, and it is used to address a loss of pigment on other areas of the body. Medical tattooing may be used as a cosmetic treatment to conceal scars from varying etiologies such as alopecic scars, vermillion scars, hypopigmented scars, and nipple-areolar reconstructive surgery after mastectomy (level of evidence: 4). A case report in 2009 detailed how a decorative tattoo was designed to conceal a scar on the abdomen from a transverse rectus abdominis (TRAM) flap procedure after breast reconstruction in a patient who had breast cancer (level of evidence: 5). , Medical tattooing may also be considered as a treatment modality for dermatologic conditions such as vitiligo (level of evidence: 4) and piebaldism (level of evidence: 4).
Eyebrow restoration via the technique of microblading was first reported by Van der Velden et al for the treatment of alopecia areata (AA) of the eyebrow in 1998 (level of evidence: 3b). , Microblading is a cosmetic procedure that is becoming increasingly popular and involves superficial micropigmentation. In microblading, the pigment is deposited into the papillary dermis using a manual device with a single needle or a blade with a varying number of stacked needles ( Pearl 7.1 ) (level of evidence: 5). ,
Scalp micropigmentation utilizes a device with one or more needles to implant metabolically inert pigment granules into the upper and midpapillary dermis, and it is this level of placement that is the determining factor for the pigment to be retained uniformly.
Indications and patient selection
SMP may be used as a noninvasive method to camouflage a variety of scalp and hair loss conditions. It is well documented that QoL in patients who experience hair loss is negatively affected ( Pearl 7.2 ). Providing a procedural intervention to conceal hair and scalp deformities through the appearance of a fuller head of hair breaks the cycle of psychological stressors that patients experience in their daily lives. After the diagnosis of a scalp or hair deformity, patients are educated on the therapeutic options that are available. In a combination treatment regimen, SMP is part of the initial treatment as the medical treatment regrows the hair, or as a permanent solution if the area to be treated is stable. SMP is not a recommended treatment modality for patients with progressive hair loss or those who change their hair color frequently. , Patients with the indications listed in Table 7.1 are the best candidates for SMP ( Pearl 7.3 ). ,
Hair loss negatively affects patient quality of life.
| Androgenetic alopecia in men |
| Female pattern hair loss |
| Scarring alopecia |
| Alopecia areata |
| Traction alopecia |
| Cosmetic (chemical) alopecia |
| Trichotillomania |
| Anagen effluvium |
| Telogen effluvium |
| Traumatic or surgical scars |
| Insufficient amount of donor hair to qualify for hair transplantation |
| Individuals who do not want to undergo hair transplantation |
| Individuals who are experiencing regional balding or thinning of hair and want the appearance of a fuller head of hair |
| Unsatisfactory coverage with medical therapy and/or hair transplantation |
Scalp micropigmentation is not a recommended treatment modality for patients with progressive hair loss or those who change their hair color frequently.
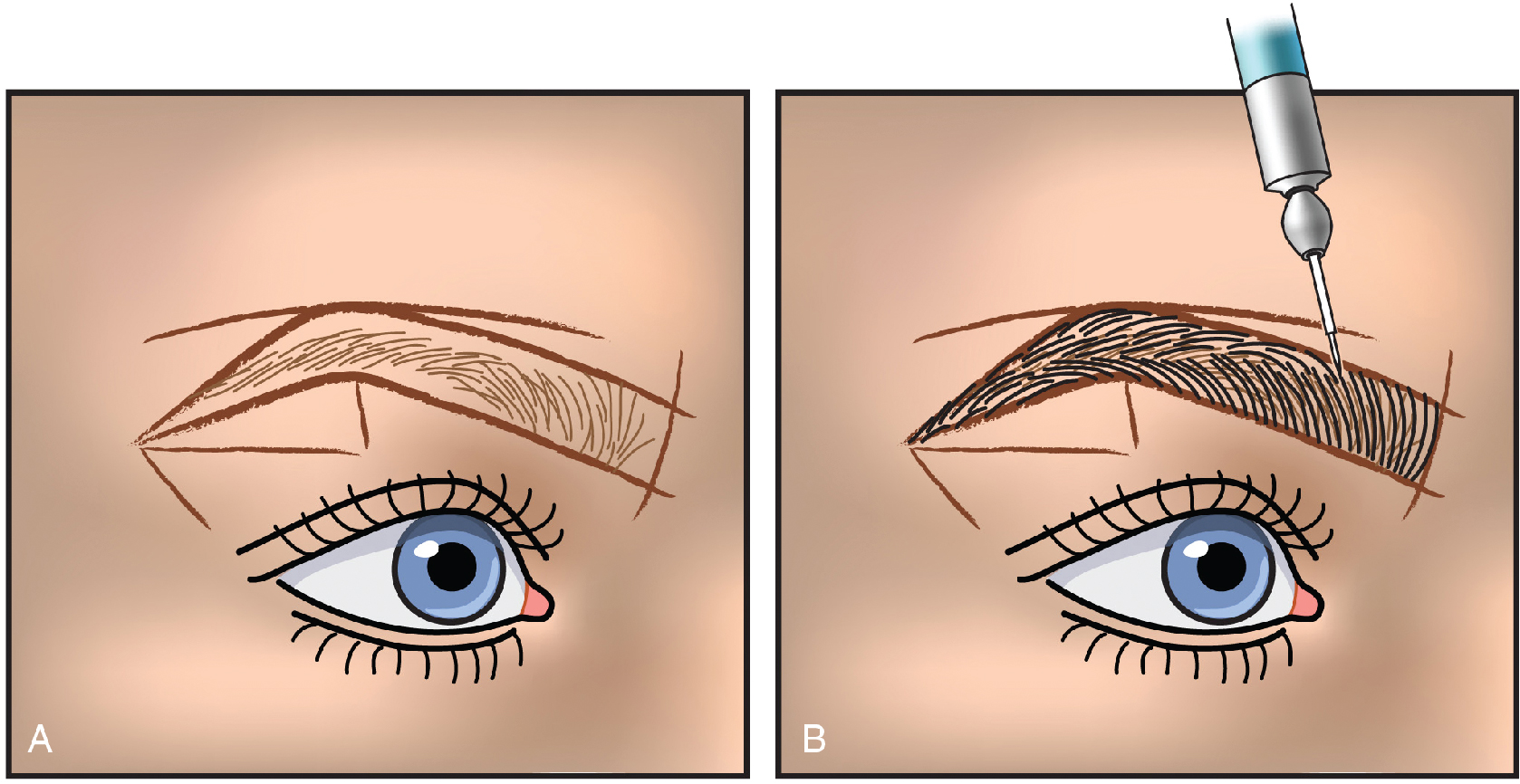
In microblading, the design of the eyebrow is dependent on the natural growth of the hair follicle ( Fig. 7.1 ). Anatomically, the eyebrow is divided into four sections: head, body, arch, and tail. These sections should be taken into careful consideration when shaping the eyebrow, as certain facial structures align best with different eyebrow variations.
At the initial consultation, it should be determined whether the patient is a good candidate for the procedure. Indications for microblading include AGA, traumatic scars, madarosis in hypothyroidism, trichotillomania, scarring alopecias (e.g., frontal fibrosing alopecia), alopecia totalis, and chemotherapy-induced hypotrichosis (level of evidence: 4). , Notable contraindications for microblading are keratosis pilaris, psoriasis, and chronic acne or oily skin, especially near the eyebrows ( Pearl 7.4 ). Providers should advise patients of the potential adverse effects associated with microblading, such as infection and contact dermatitis, as they may lead to negative outcomes in terms of patient self-esteem. , Patients should also be made aware that the pigment is semipermanent and is likely to fade over time. , Touch-ups to maintain pigment intensity are common and may be started two to three weeks after the initial procedure.
Indications for microblading include androgenetic alopecia, traumatic scars, madarosis in hypothyroidism, trichotillomania, scarring alopecias, alopecia totalis, and chemotherapy-induced hypotrichosis. Contraindications include keratosis pilaris, psoriasis, and chronic acne or oily skin near the treatment site.
Expected outcomes
A critical step for a successful SMP outcome is the selection of the proper patient for the procedure and the establishment of realistic expectations. During the initial consultation, a detailed medical history is obtained to verify whether SMP would be an appropriate procedure for the patient. At the first consult, it is important to note current medications such as blood thinners; allergies to medications; previous treatment for hair loss including medications (e.g., minoxidil, spironolactone, finasteride), scalp surgery (e.g., hair transplant, scalp reduction); and any history of relevant dermatoses (e.g., seborrheic dermatitis, psoriasis, or hypertrophic or keloid scars). The outcome the patient interprets and the work performed by the physician must be designed to align with the patient’s initial objectives. The next step is to address the areas that require coverage with SMP and to determine the total treatment surface area. In addition, the patient must be informed on approximately how long the session will last and the number of sessions needed to achieve the desired camouflaging effect. Most patients will require two to three SMP sessions at 4 to 6 week intervals ( Pearl 7.5 ). Each session is often lengthy, normally 4 to 8 hours, depending on how extensive the area of alopecia is, the presenting diagnosis, and if the treated area is normal scalp or in an area of scar tissue (level of evidence: 5). ,
Depending on the total treatment area and desired level of camouflage, most patients require two or three scalp-micropigmentation sessions. Each session may take 4 to 8 hours.
After the consultation, the scalp is evaluated to select the optimal pigment for SMP. The size of the dots or lines are assessed, and necessary adjustments are made. It is important to keep in mind that the goal is to attain results that look completely natural ( Pearl 7.6 ). The color typically stays intact for 1 to 2 years, then slowly fades with time. It is estimated that the pigment will disappear by the fifth year. If the patient consistently takes part in outdoor activities, the intensity of pigment may decrease before the estimated timeframe. To mitigate a decrease in pigment, additional sessions may be required to reinforce pigment intensity ( Pearl 7.7 ).
The goal of SMP is to attain results that look 100% natural.
Scalp micropigmentation typically fades completely after 5 years. Frequent sun exposure may cause the intensity of pigment to fade more quickly.
There are several variables that determine the outcome of SMP ( Table 7.2 ). Authors of a study involving 30 patients with AGA, cicatricial alopecia, and AA examined these variables and ideal parameters to standardize the SMP procedure and correlate it with reproducible results. Patients were assessed by clinical photography and trichoscopy at 1 month, and by clinical photography at 6 months after the SMP procedure. The treated area was evaluated by the physician using a seven-point scale and by the patient using a three-point satisfaction scale, both at 6 months. In addition, a histopathologic examination was performed to determine the ideal depth of pigment deposition. Results suggested that patients with AGA had better outcomes than those with AA or cicatricial alopecia, and that patient satisfaction was high. Adverse events included transient edema and redness.
| Angle of needle | Needle insertion at different angles |
| Depth of needle | Insertion at varying depths ranging from 0.3–1.2 mm |
| Pattern of dot placement (of pigment) | Placement of pigment in regular versus random manner |
| Tattoo ink used | Jet black versus black-brown in a ratio of 2:1 |
| Contact time of the needle | Different contact times in correlation with pigment deposition |
| Resistance of scalp | Effect of skin suppleness/elasticity/turgidity on pigment deposition |
| Speed of rotor | Effect of varying rotor speed on pigment deposition |
| Viscosity of dye | Fluidity of dye affecting outcome |
| Needle number |
|
| Level of expertise of the operator – technical and artistic skill, proper training | Length of exposure (amount of time the needle is in contact with the scalp) |
Treatment technique/best practices
Preoperative care
Preoperative instructions and the surgical instruments used for SMP are presented in Tables 7.3 and 7.4 , respectively. Preoperative photographs are recommended to document the treatment area and to monitor success of the procedure.  provides a visual of the preoperative process. The area of hair loss that will be treated should be cleansed with antiseptic and alcohol solutions ( Fig. 7.2 ), then marked with a surgical pen based on the preoperative consultation. A vibrating device is given to the patient to hold onto their chest, and two more vibrators are placed around the patient’s forehead. One of the authors (SS) uses these maneuvers to minimize the patient’s discomfort with the procedure.
provides a visual of the preoperative process. The area of hair loss that will be treated should be cleansed with antiseptic and alcohol solutions ( Fig. 7.2 ), then marked with a surgical pen based on the preoperative consultation. A vibrating device is given to the patient to hold onto their chest, and two more vibrators are placed around the patient’s forehead. One of the authors (SS) uses these maneuvers to minimize the patient’s discomfort with the procedure.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


