Key points
- •
Scarring alopecia is characterized by inflammation that leads to destruction of the pilosebaceous unit and ultimately the replacement of subcutaneous tissue with fibrous tracts. As a result, the hair loss can be disfiguring and cause significant distress in affected patients.
- •
Although treatment strategies for scarring alopecia center on disease subtype, the primary goal of treatment is to reduce the underlying inflammation causing the destruction of hair follicles to stop the progression of scarring and hair loss. Hair loss is often permanent and can have a significant psychological effect on patients, heightening the importance of establishing appropriate treatment expectations.
- •
Topical steroids, often combined with intralesional corticosteroid injections, are usually considered first-line in the treatment of scarring alopecia as a result of their demonstrated efficacy and low side-effect profile. Systemic therapies can be used for disease recalcitrant to topical and intralesional corticosteroids and are needed in most patients.
- •
Platelet-rich plasma is one of few treatment options for scarring alopecia that has demonstrated the potential for hair regrowth, even in patients who have failed conventional therapies.
- •
Surgical hair transplantation is an aesthetic treatment option that offers the unique outcome of dramatic hair restoration in scarred areas of the scalp. However, results are often variable as a result of marked fibrosis and decreased scalp vascularity in the recipient area. Caution should be taken to avoid transplantation in patients with subclinical inflammation.
Background
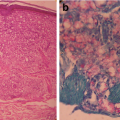
Scarring or cicatricial alopecia is a diverse class of conditions of differing etiologies and clinical presentations, in most cases leading to permanent hair loss. These disorders make up approximately 7% of patients evaluated in hair-loss specialty clinics (level of evidence: 5). Scarring alopecia can be primary, characterized by inflammation and destruction of the pilosebaceous unit with eventual replacement of subcutaneous tissue with fibrous tracts, or secondary as a result of trauma, cancer, radiation, or thermal burns (level of evidence: 5). , Primary cicatricial processes can be further classified into neutrophilic, lymphocytic, or mixed by the predominant inflammatory cell type seen on histology during the active phase of disease ( Table 3.1 ) (level of evidence: 5).
| Lymphocytic | Neutrophilic | Mixed |
|---|---|---|
|
|
|
Unlike nonscarring alopecia where the follicular unit is preserved and treatment is centered on hair regrowth, treatment for scarring alopecia is largely aimed at reducing inflammation and preventing disease progression. Consequently, hair loss can be disfiguring and may contribute to increased psychosocial burden and decreased dermatology life quality index (DLQI) scores in patients with scarring alopecia compared with those with nonscarring alopecia (level of evidence: 1b). Early diagnosis and initiation of treatment is essential for a better prognosis in these patients.
Structural and functional differences in scarring alopecia
The pilosebaceous unit consists of three anatomic structures: hair follicle, sebaceous gland, and arrector pili muscle (level of evidence: 5). The hair follicle, an epithelial organ, can further be divided into three regions: the infundibulum (uppermost segment) extending from the insertion point of the sebaceous gland to the follicular orifice; the isthmus (middle segment) extending from the entrance of the arrector pili muscle to the insertion of the sebaceous gland; and the bulb (lowermost segment) extending from the base of the hair follicle to the arrector pili muscle. Near the attachment site of the arrector pili muscle and opening of the sebaceous gland there is an area on the outer root sheath of the hair follicle called the bulge region where multipotent stem cells are located (level of evidence: 3a). , During the hair cycle, quiescent follicular stem cells are transiently activated in the early anagen (growth) phase (level of evidence: 5). These cells can proliferate and further differentiate to support elongation or regeneration of the hair shaft.
In nonscarring processes, while the histopathology is largely disease dependent, all conditions share the finding of an intact and healthy hair bulge region in early stages of disease, allowing the hair follicle to regenerate with sufficient treatment. Contrarily, scarring alopecia involves destructive inflammation around the infundibular, and variably isthmic, region of the hair follicle. This causes damage to the follicular bulge region and leads to the loss of epithelial stem cells necessary to regenerate the hair follicle (level of evidence: 2b). , With persistent inflammation, the involved tissue becomes fibrotic, resulting in permanent hair loss. The fundamental differences between scarring and nonscarring alopecia are summarized in Table 3.2 .
| Nonscarring Alopecia | Scarring Alopecia |
|---|---|
| Preservation of the pilosebaceouss unit | Destruction of the pilosebaceous unit |
| Healthy bulge region of the hair follicle with sparing of follicular stem cells | Inflammation leads to destruction of the bulge region of the hair follicle with loss of stem cells necessary for follicular regeneration |
| Absence of fibrosis | Presence of fibrosis |
| Regeneration of the hair follicle with appropriate treatment in most cases | Permanent hair loss in scapular areas of active disease in most cases |
Evaluation of scarring alopecia
Onset of scarring alopecia occurs most commonly in middle-aged adults, with only rare exceptions of familial genodermatoses developing during childhood and adolescent years (level of evidence: 5). , This may be an important distinguishing clue from some nonscarring alopecias such as alopecia areata (AA), which can affect individuals at any age (level of evidence: 2a). The threshold for a punch biopsy in patients presenting with clinical signs and symptoms concerning for a cicatricial process should remain low, as pathology examination allows for a more definitive identification of inflammatory infiltrates ( Pearl 3.1 ) . Often, two areas of the scalp are biopsied, both taken from the edge of an area of active inflammation to identify predominant cell types and provide possible insight on the underlying pathology (level of evidence: 5). However, biopsy alone may be insufficient for making an accurate diagnosis (level of evidence: 1b). A thorough patient history and clinical examination are key to establishing onset, disease course, family history, medication history, associated symptoms, and hairstyling and haircare practices. Extrascapular areas of hair growth such as the eyebrows, eyelashes, axillae, extremities, and genitalia should also be assessed, in order to establish the extent of disease involvement.
The threshold for a punch biopsy from two areas of the scalp, both taken from the edge of an active area of disease in patients presenting with clinical signs and symptoms concerning for a cicatricial process, should remain low, as pathology examination allows for a more definitive identification of inflammatory infiltrates.
On clinical examination, there are several features that may be present to allow distinction between a cicatricial and noncicatricial process. Evidence of smooth, fibrotic alopecic patches on the scalp, follicular prominence, loss of follicular ostia, perifollicular erythema or hyperkeratosis, papules, and pustules in affected areas of the scalp are several signs that may point to a scarring process (level of evidence: 5). In addition, some scarring alopecias have characteristic findings such as skin atrophy in lichen planopilaris (LPP) (level of evidence: 5) and dyspigmentation in cutaneous lupus erythematosus (level of evidence: 5).
This chapter will focus primarily on the most common cicatricial processes encountered by dermatologists and therefore the most important to understand: LPP, frontal fibrosing alopecia (FFA), and central centrifugal cicatricial alopecia (CCCA) ( Table 3.3 ).
| Lichen planopilaris (LPP) |
|
| Frontal fibrosing alopecia (FFA) |
|
| Central centrifugal cicatricial alopecia (CCCA) |
|
Lichen planopilaris
Lichen planopilaris (LPP) usually presents in adult women (level of evidence: 4). It is characterized clinically by perifollicular erythema and hyperkeratosis, with focal or diffuse alopecic patches involving the vertex and parietal scalp (level of evidence: 2b). , Careful examination of the face and extremities can provide additional evidence to support the diagnosis, as near total alopecia of the upper and lower extremities prior to the onset of scalp involvement has been described in several patients (level of evidence: 2b). Decreased or complete loss of the eyebrows is not common in this condition, but can occur (level of evidence: 5). A growing body of literature has shed light on potential disease mechanisms, including downregulation of peroxisome proliferator-activated receptor gamma (PPARG) and decreased interferon-gamma expression (level of evidence: 2b). ,
Frontal fibrosing alopecia
While histologically identical to LPP, frontal fibrosing alopecia (FFA) is considered a clinical variant as a result of its distinctive clinical presentation. , This condition primarily affects postmenopausal women between 60 and 70 years of age, but it is thought to have an earlier onset of around 40 years of age in patients of African descent (level of evidence: 2b). , Although exogenous factors such as sunscreen have been associated with disease onset, these reports have not been substantiated and remain controversial (level of evidence: 2b). , FFA characteristically presents with progressive recession of the anterior hairline, appearing as a band-like area of alopecia with sparing of isolated hairs, referred to as the “lonely hair sign” (level of evidence: 4). The clinical triad of findings in FFA are (1) pale, atrophic skin, (2) perifollicular hyperkeratosis and erythema, and (3) decreased density or complete loss of the eyebrows in 70% of patients. ,
Central centrifugal cicatricial alopecia
Central centrifugal cicatricial alopecia (CCCA) is a scarring alopecia that predominantly affects women of African descent (level of evidence: 5). CCCA presents with an insidious, centrifugal pattern of permanent hair loss beginning in the scalp vertex (level of evidence: 4). In the early stages of disease, the hair loss may present as hair breakage and thinning at the crown of the scalp. This progressively expands to involve the surrounding areas with permanent hair loss. Some patients may experience symptoms secondary to inflammation of the affected scalp, including tenderness, pruritis, scale, pustules, and papules, while others have no symptoms outside of progressive hair loss.
When first described in the literature, CCCA was referred to as “hot comb” alopecia as a result of the theory that disease onset was linked to hairstyling practices and then, later, to chemical relaxants (level of evidence: 2b). Further studies disputed any link to hot combing or chemical relaxers, and subsequent studies suggested instead a link to extensions as these styling practices became more popular (level of evidence: 2b). However, there has since been no substantial evidence to support any one hairstyling practice to the onset of CCCA, casting this hypothesis into doubt. Since a publication by Malki et al. in 2019, evidence has suggested that CCCA is an autosomal dominant condition with incomplete penetrance and is associated with variance in the PADI3 gene in 24% of patients (level of evidence: 2b). Additionally, this condition has been connected to a higher prevalence of uterine leiomyomas and type 2 diabetes, indicating potential contribution of metabolic factors in disease pathogenesis (level of evidence: 1b). ,
Treatment approaches
As stated previously, the primary goal of therapy for cicatricial alopecia is disease remission and stabilization, and this should be explicitly communicated to patients. The treatment of a primary scarring alopecia often centers on physician experience, as there is currently no gold standard approach. Early initiation of treatment is key in the proper management of these conditions to slow disease progression and address symptomatology. Response to treatment is often variable, with some patients experiencing complete resolution of symptoms and control of disease progression, while others experience persistent disease despite trial of multiple therapies.
Topical and intralesional corticosteroids
Topical potent corticosteroids, often combined with intralesional corticosteroid injections to the scalp, are generally considered a first-line therapeutic option for cicatricial alopecia. The use of topical steroids has demonstrated resolution of inflammation with no evidence of disease progression after 12 weeks of therapy in some patients (level of evidence: 4). Intralesional triamcinolone can be injected at a concentration of 5 to 10 mg/cc every six to eight weeks until clinical evidence of active inflammation, such as follicular prominence or perifollicular erythema, has resolved (level of evidence: 2b). For patients with CCCA, assessment of disease activity is more difficult, as many women do not have overt inflammation. In these patients, a series of five to eight sessions followed by a six to nine-month treatment-free period is common.
Steroid-induced atrophy, a well-known adverse effect associated with intralesional corticosteroid injections, poses an even higher risk of occurrence in patients concurrently using potent topical steroids (level of evidence: 5). Spacing out injections is essential to avoid this complication. As mentioned previously, intralesional steroid injections are generally recommended at six to eight-week intervals to reduce risk of atrophy, and potent topical corticosteroids should be used for a maximum of two-week intervals if applied daily, with a one-week break in between (level of evidence: 5) ( Pearl 3.2 ). In patients who ultimately develop pale, atrophied skin at the site of injection or topical application, further injection to the area should be avoided. Steroid-induced atrophy is typically self-limited and resolves in one to two years. However, several methods have been described to improve the appearance of atrophic areas, including the use of serial saline injections, pulsed-dye laser, and fat-grafting (level of evidence: 2b). ,
Intralesional steroid injections are generally recommended at six to eight-week intervals to reduce the risk of atrophy. Potent topical corticosteroids should be used for a maximum of two-week intervals if applied daily, with a one-week break in between.
Systemic therapies
Evidence of disease progression such as new areas of involvement or persistent inflammation despite topical and intralesional corticosteroids may prompt adjunctive treatment with oral agents. Most patients with scarring alopecia will require systemic therapy. Oral hydroxychloroquine has shown positive results in patients with LPP and FFA and can be considered as a second-line therapy, with effects seen three to six months after initiation. In the authors’ experience, patients often do well initiating oral systemic medications in addition to corticosteroid treatment. A single-center retrospective review of 40 patients with LLP and FFA found that, after 12 months, 83% of patients saw improvement in their symptoms (level of evidence: 2b). Adverse reactions associated with hydroxychloroquine use are important to monitor, as this medication can cause anorexia, abdominal pain, hematologic changes, skin hyperpigmentation, and, notably, ophthalmologic damage. These patients require annual monitoring by an ophthalmologist for the development of retinopathy.
In cases where symptoms persist on oral hydroxychloroquine after six months of treatment, mycophenolate mofetil and cyclosporine are immunosuppressive agents that can serve as alternative treatment options (level of evidence: 4). , Though oral corticosteroids offer quick control of inflammation, the rate of disease relapse in scarring alopecia has been reported to be as high as 80%. Thus, oral corticosteroids are generally not recommended, but can be reserved for cases of rapidly progressive, severe disease. , Oral tetracyclines such as doxycycline (100 mg twice daily), antiandrogens such as oral finasteride and dutasteride, and calcineurin inhibitors have been used in the treatment of CCCA refractory to other oral agents. Finasteride and dutasteride are among the most efficacious treatments for LPP and FFA, and can be used in postmenopausal women or premenopausal women who are also on a contraceptive (level of evidence: 3a). Evidence of partial hair regrowth or disease stabilization, even in severe disease, has been demonstrated in most patients (level of evidence: 2b). , Oral isotretinoin can also be used in patients with LPP and FFA to achieve disease stabilization, especially in patients with FFA who present with yellow facial papules in the early stages of disease (level of evidence: 1b).
Autologous platelet-rich plasma
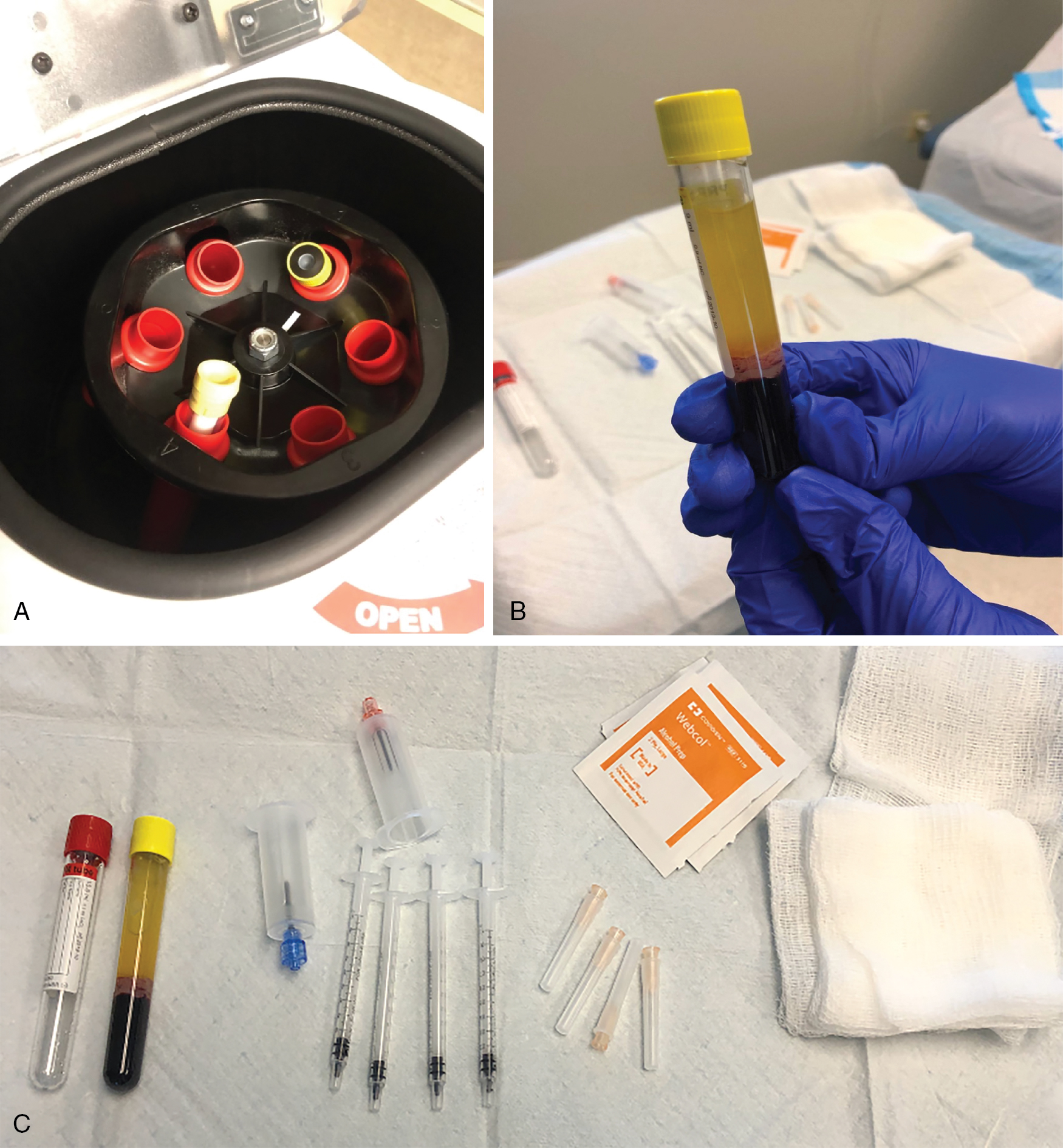
Studied since the 1970s, primarily for applications in the stimulation of wound healing, platelet-rich plasma (PRP) has recently gained traction in its aesthetic use in dermatology for the treatment of hair loss (level of evidence: 5). PRP works by enhancing cells involved in tissue regeneration such as adipose-derived stem cells and dermal fibroblasts (level of evidence: 5). The proposed mechanism of PRP stimulation of hair growth is thought to involve platelet activation that leads to a cascade of reactions and ultimately the secretion of cytokines and growth factors essential in the process of wound healing (level of evidence: 5). These growth factors then act on stem cells within the bulge region of the hair follicle, promoting neovascularization and follicular regeneration. In addition, beta-catenin and fibroblast growth factor-7 (FGF-7) activity has been found to be upregulated in patients after PRP treatment. The increased beta-catenin activity further induces proliferation of follicular stem cells, while upregulation of FGF-7 activity prolongs the anagen phase of the hair cycle to further stimulate growth.
PRP is one of the few treatments in the literature described as an option for hair restoration in patients with cicatricial alopecia. Though PRP is primarily used as an off-label treatment for nonscarring alopecia, it has also gained attention in the literature as a feasible treatment option in cicatricial alopecia with positive results ( Fig. 3.1 ). It has been described as a treatment option for patients who have failed conventional therapies, even producing positive results in patients with active, longstanding disease ( Fig. 3.2 ) (level of evidence: 4). Several case reports have been published on the use of PRP in LPP, varying from three sessions performed one month apart to four sessions administered three weeks apart (level of evidence: 4). Authors noted complete regression of inflammatory symptoms such as perifollicular erythema, hyperkeratosis, and itching, evidencing potential arrest of disease progression. Only one case report describes restoration of normal follicular density across the scalp and frontal hairline in a patient with LPP after three sessions of PRP performed one month apart. Lastly, resolution of symptomatology has also been described in FFA, with no evidence of progressive hair loss after five sessions of PRP at one-month intervals, in addition to improvement in perifollicular erythema, hyperkeratosis, and lichenoid papules present at the hairline (level of evidence: 4). It is therefore important to manage patient expectations by providing guidance on the efficacy of PRP in slowing disease progression and improving inflammation, with possible but unlikely restoration of follicular density in affected areas of the scalp.
Related posts:
 Ethnic differences in hair
Ethnic differences in hair
 Hemangiomas
Hemangiomas
 Drug eruptions
Drug eruptions
 Achieving aesthetically superior results: Tips and tricks
Achieving aesthetically superior results: Tips and tricks
 Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
Young Man with Hypopigmented Macules on Trunk and Multiple Shiny Nodules Over Face
 Human and Animal Stratum Corneum As a Partial Model for the 15 Steps of Percutaneous Absorption: Emphasizing Decontamination, Part I
Human and Animal Stratum Corneum As a Partial Model for the 15 Steps of Percutaneous Absorption: Emphasizing Decontamination, Part I
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


