Lymphedema is a chronic and progressive condition that occurs after cancer treatment. Autologous lymph node transplant, or microsurgical vascularized lymph node transfer (ALNT), is a surgical treatment option that brings vascularized vascular endothelial growth factor-C–producing tissue into the operated field to promote lymphangiogenesis and bridge the distal obstructed lymphatic system with the proximal lymphatic system. Operative techniques for upper- and lower-extremity ALNT are described with 3 donor lymph node flaps (inguinal, thoracic, cervical). Surgical technique is described for the combination of ALNT with abdominal flaps and nonabdominal flaps. Imaging showing restoration of lymphatic drainage after ALNT is shown.
- •
Autologous lymph node transplant or microsurgical vascularized lymph node transfer (ALNT) is a surgical treatment option for lymphedema, which brings vascularized, VEGF-C producing tissue into the previously operated field to promote lymphangiogenesis and bridge the distal obstructed lymphatic system with the proximal lymphatic system. Additionally, lymph nodes with important immunologic function are brought into the fibrotic and damaged tissue.
- •
ALNT can cure lymphedema, reduce the risk of infection and cellulitis, and improve brachial plexus neuropathies.
- •
ALNT can also be combined with breast reconstruction flaps to be an elegant treatment for a breast cancer patient.
Overview: nature of the problem
Lymphedema is a result of disruption to the lymphatic transport system, leading to accumulation of protein-rich lymph fluid in the interstitial space. The accumulation of edematous fluid manifests as soft and pitting edema seen in early lymphedema. Progression to nonpitting and irreversible enlargement of the extremity is thought to be the result of 2 mechanisms:
- 1.
The accumulation of lymph fluid leads to an inflammatory response, which causes increased fibrocyte activation.
- 2.
Fat deposition occurs when malfunctioning lymphatics are unable to transport fat molecules effectively.
Clinically, patients develop firm subcutaneous tissue, progressing to overgrowth and fibrosis.
Lymphedema is a common chronic and progressive condition that can occur after cancer treatment. The reported incidence of lymphedema varies because of varying methods of assessment, the long follow-up required for diagnosing lymphedema, and the lack of patient education regarding lymphedema. In one 20-year follow-up of patients with breast cancer treated with mastectomy and axillary node dissection, 49% reported the sensation of arm lymphedema. Of the patients who developed lymphedema, 77% were diagnosed within the 3-year period following breast cancer treatment, and the remaining patients developed arm lymphedema at a rate of about 1% per year after the 3 years. Therefore, about a quarter of patients will develop lymphedema years after breast cancer treatment, and a long follow-up is required.
The incidence of lymphedema after breast cancer treatment ranges from 24% to 49% after mastectomy and 4% to 28% after lumpectomy. Patients requiring more extensive breast cancer treatment with axillary node dissection and radiation have the greatest risk for the development of lymphedema. However, even the less extensive lymph dissection in sentinel node biopsy is associated with a 5% to 7% incidence of upper-extremity lymphedema.
The incidence of lymphedema after treatment of other malignancies is reported as follows: 16% with melanoma, 20% with gynecologic cancers, 10% with genitourinary cancers, 4% with head and neck cancers, and 30% with sarcoma. Patients requiring pelvic dissection and radiation therapy for the treatment of non–breast cancer malignancies have a reported lymphedema rate of 22% and 31%, respectively. Risk factors for developing lymphedema after cancer treatment are obesity, infection, and trauma.
In addition to the decreased amount of lymph tissue critical to a normal immune response, tissue changes and lymphostasis result in increased susceptibility to infection in the lymphedematous extremity. Clinically, patients may develop cellulitis from minor trauma that would otherwise be insignificant in a normal extremity ( Fig. 1 ). Each episode of infection further damages lymphatic channels and perpetuates a vicious cycle. Patients may require lifelong antibiotic prophylaxis.

Lymphedema can also lead to erysipelas, lymphangitis, and even lymphangiosarcoma. Erysipelas is a streptococcal infection of the dermis. Lymphangitis is inflammation of the lymphatic channels as a result of infection at a site distal to the channel, such as a paronychia, an insect bite, or an intradigital web space infection. Lymphangiosarcoma is a rare malignant tumor that occurs in long-standing cases of lymphedema ( Fig. 2 ). Stewart-Treves syndrome is angiosarcoma arising from postmastectomy lymphedema and has an extremely poor prognosis, with a median survival of 19 months.

Therapeutic options for iatrogenic lymphedema
Conservative Treatment
Conservative lymphedema therapy is the backbone for providing symptomatic improvement of lymphedema and may slow the progression of disease. Multiple layers of short-elastic bandages are wrapped circumferentially around the lymphedematous extremity to squeeze edema fluid out of the tissue and push the edema fluid proximally. Customized compression garments are subsequently placed on the extremity to maintain the decreased extremity size. Decongestive lymphatic therapy usually begins with intensive (daily for several weeks) lymphatic massage and bandaging. This therapy is followed by less-frequent maintenance lymphatic massage and daily placement of compression garments for the rest of patients’ lives. Flare-ups of lymphedema may require repeating the initial intensive daily lymphatic massage with bandaging. Patients with severe lymphedema may require bandaging every night and wearing compression garments everyday.
The major limitation of conservative therapy is that reduction in extremity size is short lived without continual compression; the maintenance of compression (conservative therapy) is difficult to achieve long term because it is time consuming, labor intensive, requires specialized therapists, and requires commitment of patients and patients’ support network. Frequently, it is difficult for patients to self-apply bandages. In addition, insurance companies may inadequately cover therapists for bandaging and massage therapy, requiring patients to parcel out therapy sessions. A second major limitation of conservative therapy is that it cannot affect change in extremity girth because of subcutaneous fat deposition and fibrosis. Thus, surgical options for treatment have an important role in the treatment of lymphedema, and a combination of treatment modalities may achieve the most improvement.
Surgical Treatment
Surgical options for lymphedema treatment fall into 2 categories: debulking and physiologic.
Debulking procedures may involve elliptical wedge excision of excess skin and subcutaneous tissue from an extremity or liposuction. Wedge excision of tissue can provide immediate symptomatic relief to patients with severe lymphedema. Removal of heavy or hanging bulky tissue from an extremity can improve the function of the extremity and can also improve the application of bandages and compression garments.
Liposuction is another effective modality for removing excess fat deposition as a result of abnormal lymphatic transport. It is helpful as an adjunct to other surgical treatments and can be performed in a second stage of treatment after a first-stage physiologic surgical treatment. Complications of debulking procedures may be chronic wounds, infection, widened scars, hematoma, skin necrosis, potential damage to remaining lymphatics, and worsening of the lymphedema. Compression garments are necessary lifelong after debulking methods of treatment.
Physiologic procedures seek to reconstruct the lymphatic transport system. Lympholymphatic graft is a procedure that connects an obstructed lymphatic to a healthy lymphatic using a vein or a lymphatic as an interposition graft. The procedure is technically demanding and time consuming because lymphatic channel walls are thin, transparent, and very fragile. In addition, there may be significant donor site morbidity. Lymphovenous anastomosis (LVA) connects an obstructed lymphatic to a vein to shunt the lymph fluid into the venous system and seem to be effective, especially in early stages of lymphedema. The LVA remains patent if the lymphatic pressure is higher than the venous pressure. Currently, a subdermal vein is used because it has lower venous pressure. The caliber of subdermal veins is less than a 1 mm, requiring supermicrosurgery with extrafine microsurgical instruments and sutures. Usually, multiple LVAs (3–5) are created to a lymphedematous extremity. Although in other centers, an average of 9 LVAs (range of 5–18) are routinely created by teams of surgeons operating with multiple microscopes simultaneously.
Autologous lymph node transplantation (ALNT), also called microsurgical vascularized lymph node transfer, is another reconstructive surgical treatment of lymphedema. This article focuses on ALNT and its use in patients with secondary iatrogenic lymphedema. In ALNT, a recipient bed in the lymphedematous extremity is prepared by releasing scar tissue until healthy soft tissue is encountered. Then a small flap containing superficial lymph nodes are harvested from a donor site with an artery and vein and microsurgically anastomosed to an artery and vein at the recipient site.
The ALNT procedure is considered to be physiologic for several reasons. First, scar tissue, which may be blocking lymphatic flow, is released. Second, healthy vascularized tissue in the form of a flap is brought into the previously operated site, which may bridge lymphatic pathways through the scar tissue. Third, the flap contains healthy lymph nodes, which produce vascular endothelial growth factor C (VEGF-C). VEGF-C promotes lymphangiogenesis and is hypothesized to stimulate reconnections in the distal obstructed lymphatic system with the proximal lymphatic system. Fourth, lymph nodes have important immunologic functions, and adding healthy lymph nodes may provide benefit to a lymphedematous extremity predisposed to development of infection. Fifth, lymph nodes themselves are an interface between the lymphatic and venous systems for drainage of lymph into the venous system without surgically created lymphovenous anastomoses distally on the extremity.
Therapeutic options for iatrogenic lymphedema
Conservative Treatment
Conservative lymphedema therapy is the backbone for providing symptomatic improvement of lymphedema and may slow the progression of disease. Multiple layers of short-elastic bandages are wrapped circumferentially around the lymphedematous extremity to squeeze edema fluid out of the tissue and push the edema fluid proximally. Customized compression garments are subsequently placed on the extremity to maintain the decreased extremity size. Decongestive lymphatic therapy usually begins with intensive (daily for several weeks) lymphatic massage and bandaging. This therapy is followed by less-frequent maintenance lymphatic massage and daily placement of compression garments for the rest of patients’ lives. Flare-ups of lymphedema may require repeating the initial intensive daily lymphatic massage with bandaging. Patients with severe lymphedema may require bandaging every night and wearing compression garments everyday.
The major limitation of conservative therapy is that reduction in extremity size is short lived without continual compression; the maintenance of compression (conservative therapy) is difficult to achieve long term because it is time consuming, labor intensive, requires specialized therapists, and requires commitment of patients and patients’ support network. Frequently, it is difficult for patients to self-apply bandages. In addition, insurance companies may inadequately cover therapists for bandaging and massage therapy, requiring patients to parcel out therapy sessions. A second major limitation of conservative therapy is that it cannot affect change in extremity girth because of subcutaneous fat deposition and fibrosis. Thus, surgical options for treatment have an important role in the treatment of lymphedema, and a combination of treatment modalities may achieve the most improvement.
Surgical Treatment
Surgical options for lymphedema treatment fall into 2 categories: debulking and physiologic.
Debulking procedures may involve elliptical wedge excision of excess skin and subcutaneous tissue from an extremity or liposuction. Wedge excision of tissue can provide immediate symptomatic relief to patients with severe lymphedema. Removal of heavy or hanging bulky tissue from an extremity can improve the function of the extremity and can also improve the application of bandages and compression garments.
Liposuction is another effective modality for removing excess fat deposition as a result of abnormal lymphatic transport. It is helpful as an adjunct to other surgical treatments and can be performed in a second stage of treatment after a first-stage physiologic surgical treatment. Complications of debulking procedures may be chronic wounds, infection, widened scars, hematoma, skin necrosis, potential damage to remaining lymphatics, and worsening of the lymphedema. Compression garments are necessary lifelong after debulking methods of treatment.
Physiologic procedures seek to reconstruct the lymphatic transport system. Lympholymphatic graft is a procedure that connects an obstructed lymphatic to a healthy lymphatic using a vein or a lymphatic as an interposition graft. The procedure is technically demanding and time consuming because lymphatic channel walls are thin, transparent, and very fragile. In addition, there may be significant donor site morbidity. Lymphovenous anastomosis (LVA) connects an obstructed lymphatic to a vein to shunt the lymph fluid into the venous system and seem to be effective, especially in early stages of lymphedema. The LVA remains patent if the lymphatic pressure is higher than the venous pressure. Currently, a subdermal vein is used because it has lower venous pressure. The caliber of subdermal veins is less than a 1 mm, requiring supermicrosurgery with extrafine microsurgical instruments and sutures. Usually, multiple LVAs (3–5) are created to a lymphedematous extremity. Although in other centers, an average of 9 LVAs (range of 5–18) are routinely created by teams of surgeons operating with multiple microscopes simultaneously.
Autologous lymph node transplantation (ALNT), also called microsurgical vascularized lymph node transfer, is another reconstructive surgical treatment of lymphedema. This article focuses on ALNT and its use in patients with secondary iatrogenic lymphedema. In ALNT, a recipient bed in the lymphedematous extremity is prepared by releasing scar tissue until healthy soft tissue is encountered. Then a small flap containing superficial lymph nodes are harvested from a donor site with an artery and vein and microsurgically anastomosed to an artery and vein at the recipient site.
The ALNT procedure is considered to be physiologic for several reasons. First, scar tissue, which may be blocking lymphatic flow, is released. Second, healthy vascularized tissue in the form of a flap is brought into the previously operated site, which may bridge lymphatic pathways through the scar tissue. Third, the flap contains healthy lymph nodes, which produce vascular endothelial growth factor C (VEGF-C). VEGF-C promotes lymphangiogenesis and is hypothesized to stimulate reconnections in the distal obstructed lymphatic system with the proximal lymphatic system. Fourth, lymph nodes have important immunologic functions, and adding healthy lymph nodes may provide benefit to a lymphedematous extremity predisposed to development of infection. Fifth, lymph nodes themselves are an interface between the lymphatic and venous systems for drainage of lymph into the venous system without surgically created lymphovenous anastomoses distally on the extremity.
Indications for ALNT in iatrogenic lymphedema
Iatrogenic lymphedema is most commonly associated with the treatment of cancer, such as lymph node dissection and radiation therapy. Alternatively, lymphedema may also be caused by nononcologic procedures, such as saphenous vein removal, hernia repair, liposuction, and thigh lift. When lymphedema is caused by previous surgery, a lymph node flap may be indicated to reconstruct the deficit.
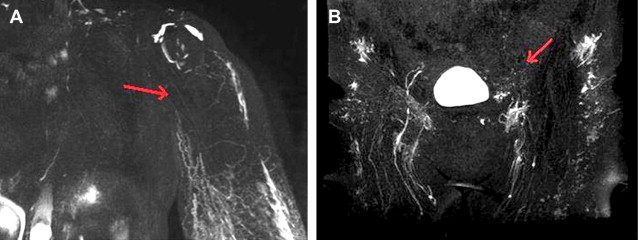
A complete blockage of lymph drainage pathways from removal and/or damage to lymph nodes is an absolute indication for ALNT to replace the missing or damaged lymphatic tissue. This condition can be diagnosed on lymphoscintigraphy as a lack of uptake of a radioactive particle (technetium-99 m) in the inguinal or axillary lymph nodes after distal injection of the particle in the extremity. More recently, magnetic resonance lymphography (MRL) with T2-weighted images, also called lymphatic magnetic resonance imaging (MRI), is being used to visualize the lymphatic system anatomy with greater sensitivity. An absence of lymph nodes and/or lymph channels traversing the surgical site may appear as a black area on MRL ( Fig. 3 ).
Related posts:
 Are We Witnessing the Emergence of a Superspecialty?
Are We Witnessing the Emergence of a Superspecialty?
 Applications of Biomaterials in Plastic Surgery
Applications of Biomaterials in Plastic Surgery
 Impact of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Impact of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


