Medication-Induced Hypersensitivity Reactions
Grace L. Lee
Barbara Reichert
Alejandro A. Gru
Benjamin H. Kaffenberger
Medication-induced hypersensitivity reactions are an important cause of morbidity, and even mortality within the pediatric population. Fortunately, they tend to be less frequent than those seen in adults, likely related to fewer medications concurrently used.1 Dermatopathology plays an important role in distinguishing low-risk idiosyncratic drug eruptions from high-risk immunologic reactions. In addition to the risks of severe toxicity, if the diagnosis is not properly made, medical and economic costs can be substantial with misdiagnoses.2 The causative drug often will not be apparent by histopathology and clinicians should be directed to validate criteria to assess the etiology such as the Naranjo or Alden scores.3,4 This chapter distinguishes three general drug eruption presentations: the classic idiosyncratic drug reactions, chemotherapy and targeted oncologic associated eruptions, and severe cutaneous adverse reactions.
Classic Idiosyncratic Drug Reactions
Classic idiosyncratic eruptions in this chapter will focus on immediate-type reactions (or urticarial), serum sicknesslike reactions, morbilliform eruptions, fixed drug eruptions, and acneiform eruptions. Epidemiologically, these five form the majority of typical drug eruptions, particularly in the hospital setting where the morbilliform eruption will be, by far, the most common.5,6,7,8 Children produce a unique challenge in that these eruptions can often mimic viral hypersensitivity reactions that are far more frequent compared to adults. Fortunately, children tend to be on fewer medications than adults, which allows easier evaluation of drug causality.
IMMEDIATE-TYPE URTICARIAL HYPERSENSITIVITY REACTION
Definition and Epidemiology
Etiology
Immediate-type hypersensitivity reactions occur because of preformed immunoglobulin E autoantibodies recognizing the drug, excipient, or metabolite. Any medicine can be a potential cause, although antibiotics tend to have the highest risk.
Clinical Presentation
Classically, this will present as near-immediate urticarial plaques developing across the body, often times with arcuate, annular, or figurate appearances (Figure 28-1). Pruritus is common, although scale should not be seen. Patients can also have associated angioedema, including periocular, hand, and perioral edema, and may be accompanied by oral swelling, wheezing, and anaphylaxis. In the absence of angioedema, the eruptions will often clear within hours to a few days of stopping the offending medication.
 FIGURE 28-1. Urticaria: scattered erythematous, edematous papules, and plaques over the upper body. |
Histologic Findings
Microscopically, the stratum corneum and epidermis will not demonstrate any irregularity and only minimal spongiosis. Dermal edema can be prominent, with a sparse perivascular infiltrate of lymphocytes with or without mast cells and eosinophils.11 Upon close examination of the vessels, marginating neutrophils may be seen.
Differential Diagnosis
Urticaria can be challenging and be confused with normal skin when there is minimal edema. However, the lack of interface dermatitis and minimal perivascular lymphocyte extravasation should differentiate urticaria from a morbilliform drug eruption. Urticarial vasculitis is another consideration, but should show typical features of fibrinous necrosis of the vessel walls and more extensive red blood cell extravasation.
CAPSULE SUMMARY
IMMEDIATE-TYPE URTICARIAL HYPERSENSITIVITY REACTION
Urticaria is one of the most common types of drug reactions, but often will be obvious to the clinician on the basis of appearance and time course. Pathologically, it will be characterized by a lack of injury to the epidermis, with dermal edema, and marginating neutrophils within the superficial blood vessels.
SERUM SICKNESS-LIKE REACTION
Definition and Epidemiology
Serum sickness itself is a rare condition typically associated with infusion of foreign proteins such as horse antithymocyte globulin. It is the classic type 3 hypersensitivity reaction involving immune complex development and tissue deposition resulting in hypocomplementemia, urticaria, vasculitis, fever, arthralgia, and often kidney damage. Serum sickness-like reactions are characterized by urticaria, arthritis, and fever, but do not have life-threatening risks that true serum sickness does.
Serum sickness is very rare. Serum sickness-like reactions are reported at less than 1% of all drug eruptions and primarily in children under 5.12
Etiology
In clinical practice, cefaclor is the most common medication associated with this reaction pattern. Other rarely reported etiologies include other cephalosporins, penicillins, minocycline, infliximab, and insulin.13 Interestingly, unlike true serum sickness, serum sickness-like reactions tend to be triggered most often by small molecules and not proteins.
Clinical Presentation
Patients present with urticarial eruption, arthritis, and fevers,14 which resolve upon drug withdrawal, without long-term complications. The eruption tends to occur 1 to 3 weeks after starting the therapy, in contrast to immediate-type hypersensitivity eruptions.
Histologic Findings
The histology is generally indistinguishable from common urticaria and thus it is imperative for the clinician to recognize that the fevers and arthralgias are not typical for a simple urticarial eruption.
Differential Diagnosis
Urticaria must be distinguished clinically. Urticarial vasculitis should be distinguished by the fibrinoid vessel wall necrosis, and may be concerning for true serum sickness if the patient has been treated with foreign proteins. Systemic lupus erythematosus and juvenile idiopathic arthritis are considerations in a young patient presenting with arthralgias, fevers, and rashes, but the pathology should distinguish these cases, without interface pattern changes. Viral hypersensitivity reactions would also be in the differential, particularly parvovirus and Epstein-Barr virus, but generally the clinician should recognize the eruption as fixed and thus not urticarial, in these cases. Pathologically, more interface dermatitis and superficial lymphocyte infiltration should be seen instead of urticarial features.
CAPSULE SUMMARY
SERUM SICKNESS-LIKE REACTION
Serum sickness-like reactions are rare eruptions that should be distinguished from true serum sickness. They are most often seen in children associated with antibiotics, such as cefaclor, and consist of the triad of urticarial eruption, arthralgias, and fevers.
MORBILLIFORM DRUG ERUPTION (MACULOPAPULAR/EXANTHEMATOUS)
Definition and Epidemiology
Etiology
Morbilliform drug eruptions present after metabolite or other drug-antigen internalization, and presentation to the lymphocytes resulting in a specific delayed-type reaction. Many medications can cause this eruption, but antibiotics, particularly penicillins, cephalosporins, sulfa antibiotics, and aromatic antiepileptics most commonly are associated.
Clinical Presentation
The eruption typically begins on the trunk as scattered, small erythematous blanching papules (Figure 28-2). Over the next several days, these papules progress in a centrifugal pattern. Centrally, the papules fade to macules and coalesce into patches. This eruption generally does not affect the face, palms/soles, cause lymphadenopathy, nor is it associated with an enanthem. These features would be suspicious for severe cutaneous adverse reactions or a viral etiology.16,17
Histologic Findings
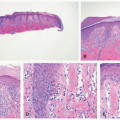
The histology of these eruptions is not specific, but typically the inflammation is perivascular and is confined to superficial dermis, containing lymphocytes with or without eosinophils and neutrophils (Figure 28-3).18 A total of 50% of cases may have associated interface changes, and similarly, only 50% of cases have eosinophils present in the inflammatory infiltrate.15
Differential Diagnosis
The differential diagnosis contains other causes of drug eruptions, viral hypersensitivity reactions, severe cutaneous adverse drug reactions, and graft-versus-host disease. Unfortunately, quantitating eosinophils in the inflammatory infiltrates has not been associated with differentiation of these hypersensitivity reactions or in distinguishing graft-versus-host disease;19,20 thus it is imperative for clinicopathologic correlation for the final diagnosis.
 FIGURE 28-2. Morbilliform eruption: coalescing macules and papules over the trunk and spreading to the extremities. The etiology in this case was a cephalosporin antibiotic. |
CAPSULE SUMMARY
MORBILLIFORM DRUG ERUPTION
Morbilliform eruptions are the most commonly diagnosed form of drug eruptions. Pathologically, they are characterized by superficial perivascular inflammation potentially with interface dermatitis, but at present, drug, viral, or graft-versus-host disease cannot be differentiated reliably without clinicopathologic correlation.
FIXED DRUG ERUPTION
Definition and Epidemiology
Fixed drug eruption is a recurrent, perfectly annular, eruption that will reoccur in the exactly same location with repeated ingestion of the offending medication.
Etiology
This is another form of a delayed-type hypersensitivity reaction, but one where cytotoxic T cells are the primary effector cell.21 The most common causes for fixed drug eruptions are terbinafine,-azole antifungals, trimethoprim-sulfamethoxazole and sulfa drugs, penicillin and cephalosporin antibiotics, tetracycline antibiotics, nonsteroidal anti-inflammatory drugs, and over-the-counter decongestants.22
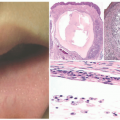
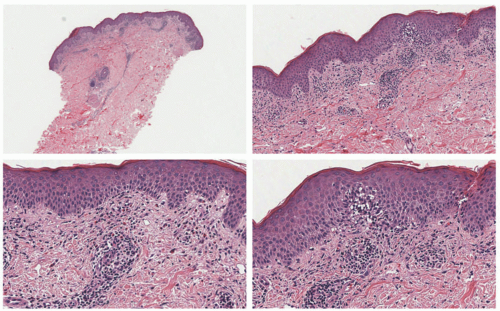 FIGURE 28-4. Fixed drug reaction; a lichenoid/interface dermatitis is prominent. There is a vacuolar degeneration of basal keratinocytes and frequent dyskeratotic cells. Pigment incontinence in the dermis is noted. The dermal inflammatory infiltrate also shows the presence of eosinophils. Digital slides courtesy of Path Presenter.com. |
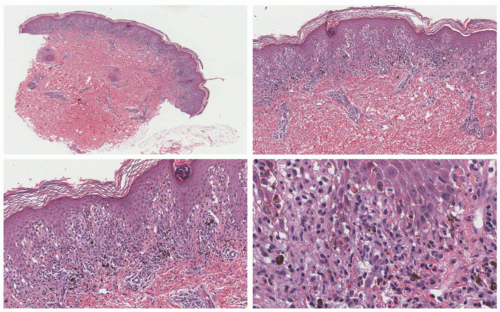 FIGURE 28-3. Morbilliform reaction—histopathologic findings. A mild degree of spongiosis and acanthosis is noted. The more prominent manifestations are in the dermis, where a superficial and perivascular inflammatory infiltrate is noted, with numerous dermal eosinophils. Focal interface changes are present (bottom right panel). Digital slides courtesy of Path Presenter.com. |
Clinical Presentation
Fixed drug eruptions almost always present as a single or multiple, clustered, perfectly annular, sharply demarcated, dusky, erythematous patches. Patients will generally describe burning as opposed to itching.21 The most common locations are the perioral skin, dorsal hands and feet, and glans penis. Occasionally, the eruption can generalize, but typically can still be distinguished from Stevens-Johnson syndrome by the lack of significant mucosal involvement.
Histologic Findings
Pathologically, this eruption will look very similar to that of Stevens-Johnson syndrome with an interface dermatitis and keratinocyte necrosis that can be full thickness. In contrast to Stevens-Johnson syndrome, eosinophils may be more abundant, and often pigment dropout and melanophages will be visible from a previous reaction (Figure 28-4).
Differential Diagnosis
The consistent locations and rapid onset after drug use should be highly supportive of the diagnosis. However, erythema multiforme (EM) may also present similarly clinically. Histologically, it may not be distinguishable if the pigment dropout is not present. Stevens-Johnson syndrome and EM should be ruled out with clinicopathologic correlation by the locations of involvement, targetoid versus homogeneous patches, microorganism etiology (EM), and by substantial mucosal involvement.
CAPSULE SUMMARY
FIXED DRUG ERUPTION
Fixed drug eruptions are another common idiosyncratic eruption. Pathologically, they look very similar to those of EM or Stevens-Johnson syndrome, but they may be distinguished by tissue eosinophils and melanophages.
ACNEIFORM ERUPTION
Definition and Epidemiology
Acneiform eruption is a follicle-based pustular eruption over the upper body, head, and neck triggered by a drug. This eruption is generally considered rare or is not lumped with other causes of drug eruptions, except in the case of epidermal growth factor inhibitors, where the incidence of papulopustular eruptions can be as high as 90% of patients.23,24,25,26
Etiology
Acneiform eruptions may occur from many different etiologies, especially corticosteroids, lithium, and hormone supplements.27 The similar papulopustular eruption of epidermal growth factor inhibitors, and mammalian target of rapamycin inhibitors is common and is addressed in the section on cancer.
Clinical Presentation
Papules and pustules over the upper chest and back, and most dense over the face and neck. Typically, comedones are not seen.
Histologic Findings
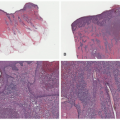
A follicular-based pustule or multiple pustules, folliculitis, and ruptured follicular structures are the typical features seen in acneiform drug reactions. (Figure 28-5). Usually, the follicles will not have significant bacterial or yeast colonization, although demodex may be present.
Differential Diagnosis
Acute generalized exanthematous pustulosis and diseases of subcorneal pustules need to be distinguished from the follicular pustules in this type of drug eruption. Demodex and malassezia folliculitis could also be considered if there is a high density of organisms in the follicles. Lastly, normal adolescent acne could be a mimicker, but typically children will notice the flare with one of the common etiologies of this eruption.
CAPSULE SUMMARY
ACNEIFORM ERUPTION
Acneiform eruption is a papular and pustular drug eruption that does not coalesce like the other drug eruptions. Typically, the eruption does not contain comedones, and the extent of the follicular inflammation should distinguish this eruption from acute generalized exanthematous pustulosis (AGEP) and other subcorneal pustular diseases.
CUTANEOUS ADVERSE EVENTS ASSOCIATED WITH TUMOR NECROSIS FACTOR INHIBITION
Definition and Epidemiology
A spectrum of toxicities, including paradoxical skin inflammation, psoriasis, palmoplantar eczema, cutaneous lupus, as well as infusion reactions can be seen with tumor necrosis factor inhibitors. Overall, these reactions are not infrequent. Paradoxical skin disease of psoriasis, eczematous, or other inflammatory skin diseases occurs in 5% to 10% of patients undergoing treatment with tumor necrosis factor (TNF) inhibitors for inflammatory bowel disease, whereas the rate is only 0.1% among patients treated for rheumatoid arthritis.28 Including events such as infusion and injection site reactions, dermatologic toxicities can occur in 25% of patients.29
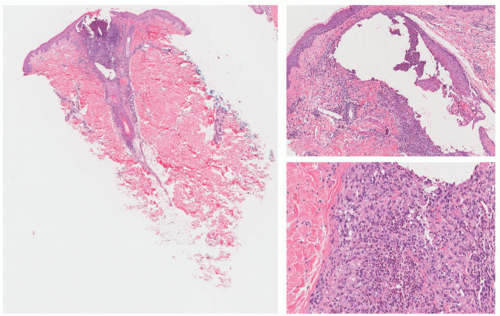 FIGURE 28-5. Acneiform eruption in association with epidermal growth factor receptor inhibitors. A pustular folliculitis and perifolliculitis is present. At the edges of the inflamed follicle, focal granulomatous changes are present. |
Etiology
Clinical Presentation
The presentations are highly variable. Most commonly, psoriasis, generally of the palmoplantar subtype, dermatitis, or drug-induced lupus are reported. Less common presentations include vasculitis with palpable purpura or cutaneous lymphoma.30 These diseases generally mimic classic forms of disease, with a preponderance of palmoplantar involvement. TNF-associated lupus may or may not affect the skin.31 Infusion reactions occur only in patients receiving infusions, such as infliximab, and present cutaneously with an urticarial eruption or angioedema. Injection site reactions are highly variable on the basis of the therapy but tend to present with injection site pain and short-lived erythema.
Histologic Findings
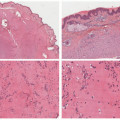
Similarly, the histopathology of these diverse eruptions will mimic their classic forms of skin disease (Figure 28-6): psoriasiform forms are typical with regular elongation of the rete, intracorneal collections of neutrophils, superficial papillary dermal vessel dilatation, and a decreased granular cell layer. Other drug reactions can show features of pustular psoriasis or AGEP. As opposed to the classic forms of psoriasis, dermal eosinophils are frequently seen.
Differential Diagnosis
The differential diagnosis includes the same skin diseases developing in a de novo fashion; however, the recent initiation of a TNF inhibitor should trigger the consideration of a paradoxical immune effect.
CAPSULE SUMMARY
CUTANEOUS ADVERSE EVENTS ASSOCIATED WITH TUMOR NECROSIS FACTOR INHIBITION
There are many paradoxical skin diseases associated with the TNF inhibitors. With the frequency of use in children with inflammatory bowel disease and arthropathies, dermatologists should be aware of the various immune-mediated events. Whether the TNF inhibitor is changed, stopped, or continued, children who have developed psoriasis tend to partially or completely clear primarily with topical corticosteroids.32
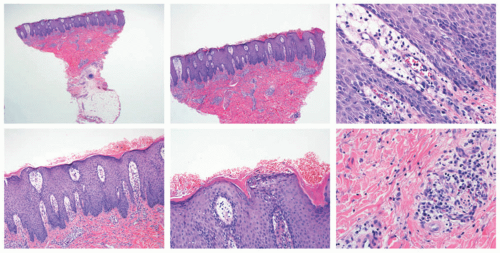 FIGURE 28-6. Psoriasiform drug reaction in association with tumor necrosis factor blockers. Psoriasiform epidermal acanthosis with regular elongation of the rete is seen. Dilatation of the superficial papillary dermal vessels is also present. Within the stratum corneum and superficial epidermis, collections of neutrophils are seen. Within the dermis, scattered eosinophils are seen, more numerous in number to what could be seen in cases of psoriasis. |
Cutaneous Toxicity Reactions From Chemotherapeutic Agents in Children
Cancer remains the second leading cause of death in children aged 5 to 14 years, with accidents being the leading cause.33 The top five most common cancers in children are acute lymphoblastic leukemia, brain and central nervous system tumors, neuroblastoma, non-Hodgkin lymphoma (particularly anaplastic lymphoma kinase + anaplastic large cell lymphoma), and Wilms tumor.33 Chemotherapeutic agents can be effective, but may cause cutaneous adverse reactions; the most common are addressed in the following section.
TOXIC ERYTHEMA OF CHEMOTHERAPY
Definition and Epidemiology
Chemotherapy can cause direct cytotoxic cutaneous toxicity. Toxic erythema of chemotherapy is a clinical term that encompasses a spectrum of reactions, including acral erythema, eccrine squamous syringometaplasia, malignant intertrigo,34 and neutrophilic eccrine hidradenitis (chemotherapy-induced) among others.35 These reactions favor acral sites, intertriginous areas (particularly the scrotum), and also elbows and knees.35
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


