Introduction
Mastopexy is the surgical technique mostly employed for modification of volume, compaction, and repositioning of the breast mound. The harmonious combination of proportion, position, and projection requires a dermoglandular resection or, sometimes, exclusively skin resections, resulting in extensive scarring. The balance between breast shape and scarring has long posed a challenge to the plastic surgeon in search for lesser incisions that do not change the breast morphology. Periareolar mastopexy allows resection, compaction, and repositioning of the breast mound, providing wide surgical access, reduced scarring, and long-term stable results in specific cases.
The senior author’s experience in the field of breast-conserving surgery for breast cancer led him to explore the concept of using the periareolar approach in aesthetic breast surgery. In 1976, Dr. J.C. Góes described the resection of a breast quadrant by the periareolar approach and reconstruction of the resulting defect by approximating the glandular flaps. This technique was the basis for the description of periareolar mammaplasty, first published in 1989. , The surgical technique was initially designed to reduce and reshape the breast for a more harmonious appearance. At that time, synthetic mesh interposition was not used for the stability of the aesthetic outcome. Instead, de-epithelialized periareolar skin excess was used as an internal “brassiere” to support the reshaped breast. However, this type of support was insufficient to provide a stable breast contour in the long term.
A mesh support was then innovated and was interposed between the reshaped breast mound and the skin flap to prevent tissue distention in the distal direction. Tissue stretch leads to widening of the breast base and areola, resulting in loss of aesthetic results in the short and medium term. The use of a mesh support provides long-lasting aesthetic results by helping maintain the proportion and position of the reshaped breast, allowing adequate tissue fixation, and counterbalancing healing forces and gravity.
Meshes of different materials have been used as a support system. First, a polyglactin 910 mesh was employed, because this is a fully absorbable mesh, but changes of aesthetic outcome were observed 2–3 years after surgery. , As a result, partially absorbable meshes started to be used as a support system, resulting in longer lasting aesthetic results. ,
This chapter describes the refinements incorporated in the technique over the years, making periareolar mastopexy a treatment of choice for achieving satisfactory and long-lasting results in patients with mild to moderate breast ptosis and hypertrophy.
Indications and Contraindications
The parameters for indication of periareolar mastopexy include the degree of breast hypertrophy, degree of ptosis, quality of breast tissue (glandular and adipose tissue), and thickness and laxity of the skin. Thus the technique is particularly indicated in cases of mild to moderate breast ptosis, breast hypertrophy requiring up to 500 g resection per breast.
The surgical access via periareolar incision broadens the indications for breast-conserving surgery in the treatment of breast cancer, allowing breast reconstruction with preservation of the mammary gland structure, even after extensive resection. The technique is also a good alternative for correction of breast asymmetry resulting from oncologic surgery.
Patients with a history of any previous breast procedure, those showing signs of transient poor perfusion of the nipple–areola complex (NAC), and smokers should not undergo periareolar mastopexy, as described in this chapter.
Preoperative Evaluations and Special Considerations
A careful patient selection is fundamental for obtaining predictable and satisfactory results. The quality of breast tissue is an important selection criterion to be considered. Patients with a thicker dermal layer and greater skin elasticity experience a more efficient retraction and better tissue adaptation during wound healing, resulting in an aesthetically acceptable scar. In addition, long-lasting results are associated with breasts containing a large proportion of glandular tissue, which results in increased stability to the breast mound ( Box 13.1 ).
- •
Mild to moderate ptosis
- •
Resection of breast tissue less than 500 g
- •
Breast-conserving surgery for breast cancer
- •
Correction of breast asymmetry
- •
Breasts with a large proportion of glandular tissue
- •
Adequate thickness and elasticity of the skin
Surgical Techniques
Preoperative Marking
The preoperative marking of the periareolar area to be de-epithelialized must be rigorously planned to ensure balance among breast proportion, position, and projection after surgery. Resections leading to excessive tension on the suture line result in loss of breast projection and widening of the areola and scar.
The marking is based on four anatomic landmarks, as follows:
- 1.
Sternal notch
- 2.
Inframammary fold (IMF)
- 3.
Midsternal line
- 4.
Outer edge of the breast
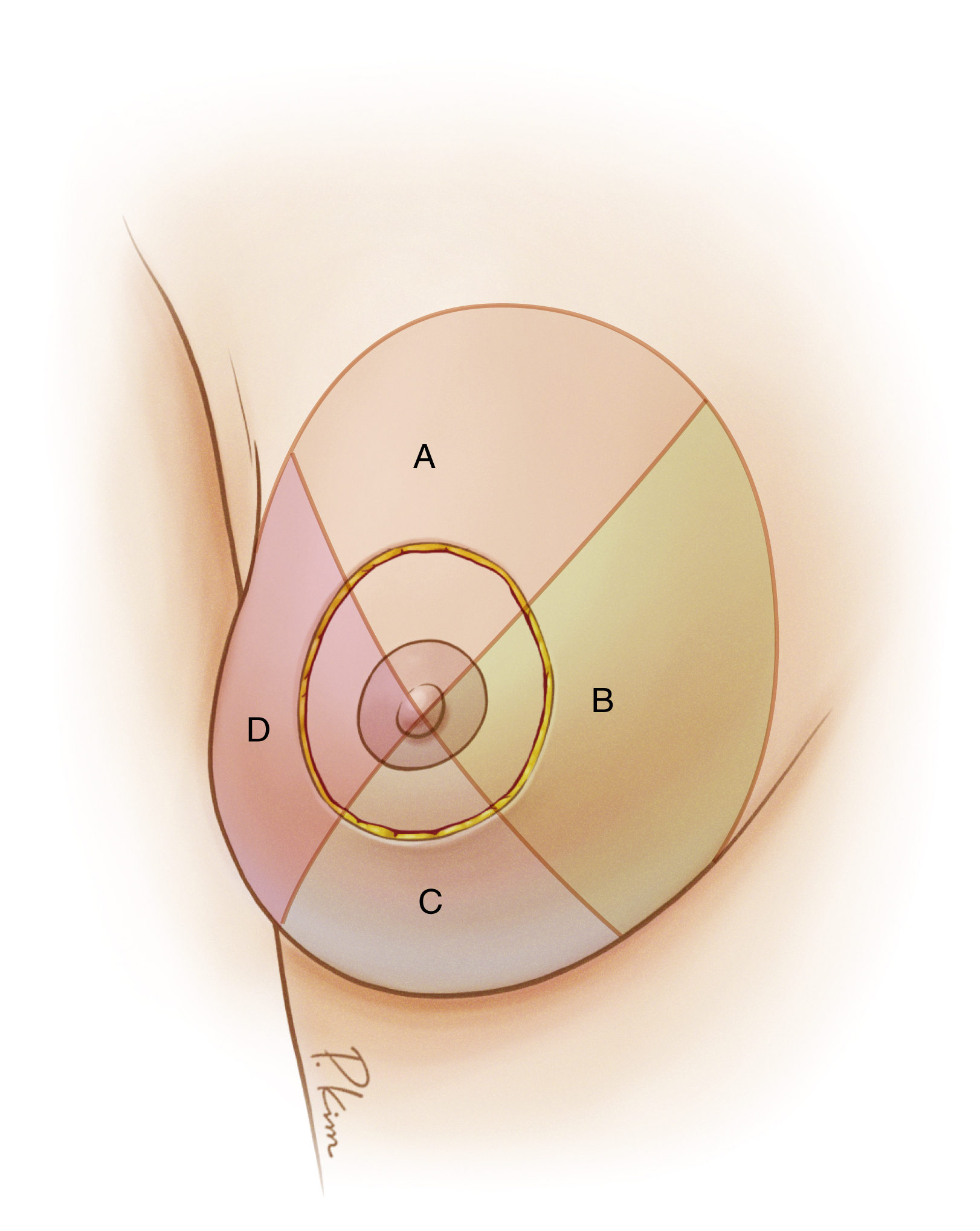
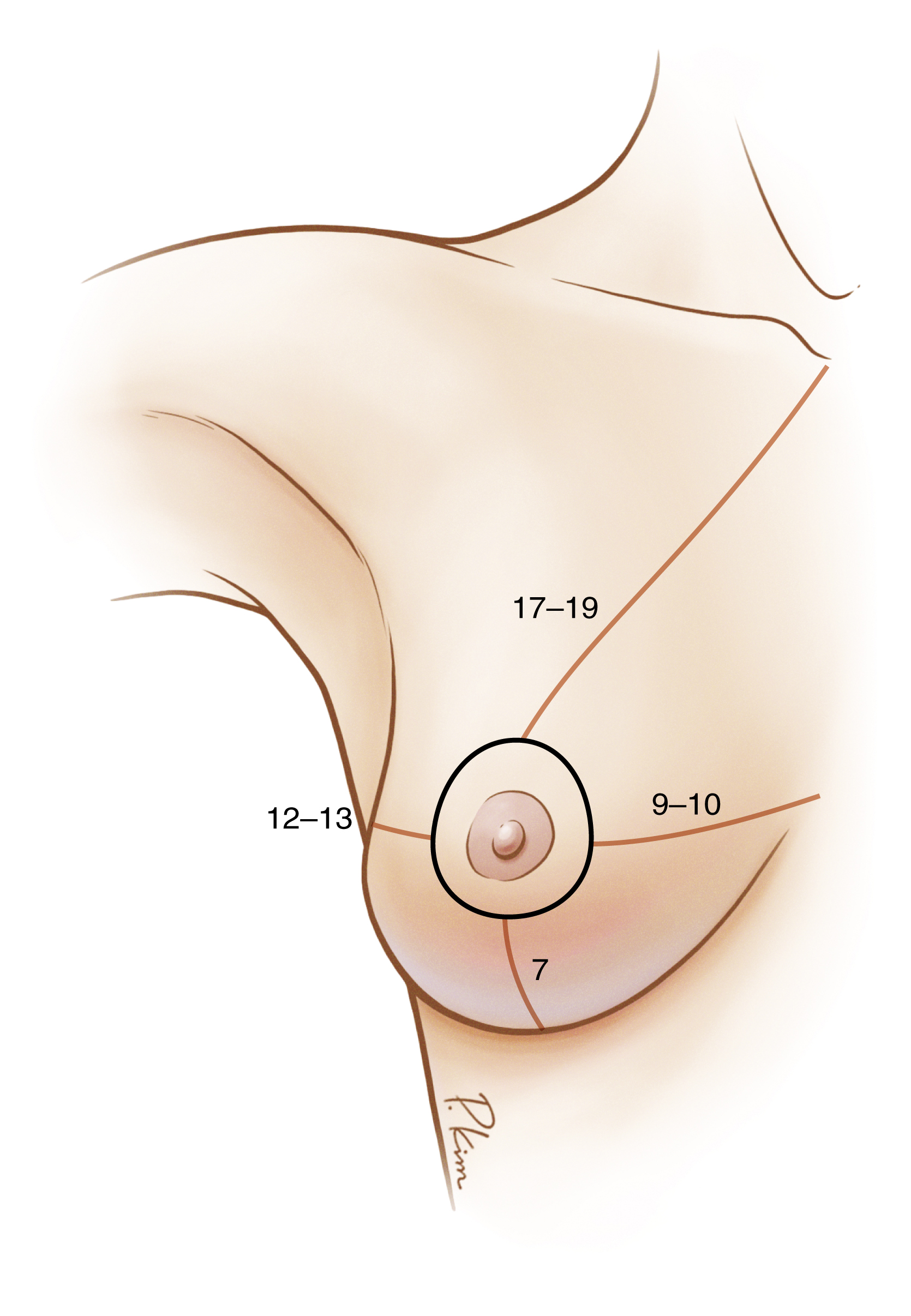
Point A represents the final position of the upper edge of the NAC and is marked approximately 17–19 cm from the sternal notch. Point B corresponds to the final position of the lower edge of the NAC and is placed 7 cm from the IMF. Points A and B define the vertical axis of the breast, responsible for the elevation of the NAC and definition of the breast mound. Point C marks the final position of the inner edge of the NAC and is located about 9–10 cm from the midsternal line. Point D refers to the final position of the outer edge of the NAC and is marked 12–13 cm from the outer edge of the breast or anterior axillary line. Points C and D define the transverse axis of the breast ( Figs. 13.1 and 13.2 ).
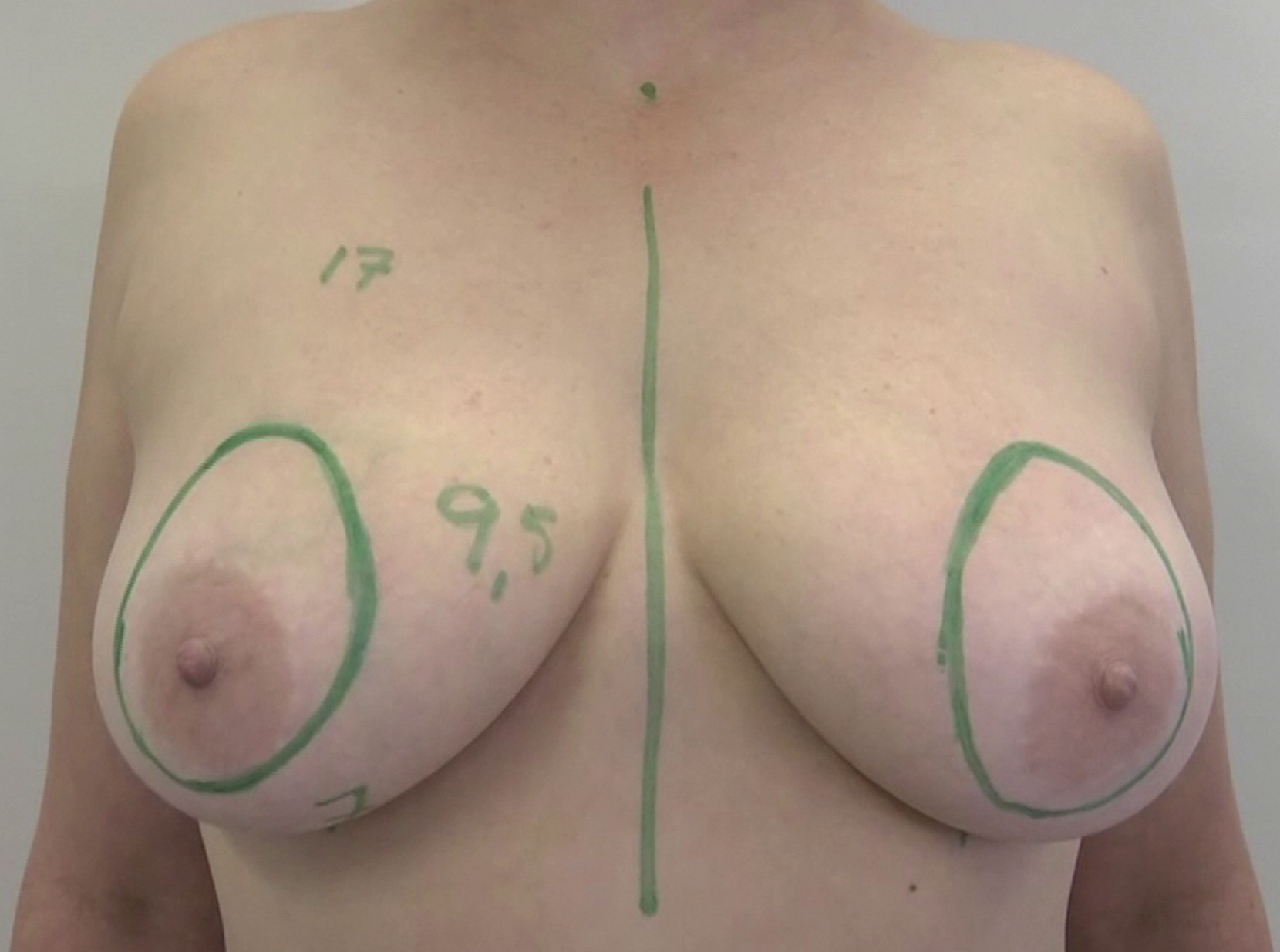
Special attention should be given to the final checking of the surgical marking by manually testing tissue approximation, especially in the transverse axis, to prevent excessive resection of skin, which may affect breast shape and scar quality.
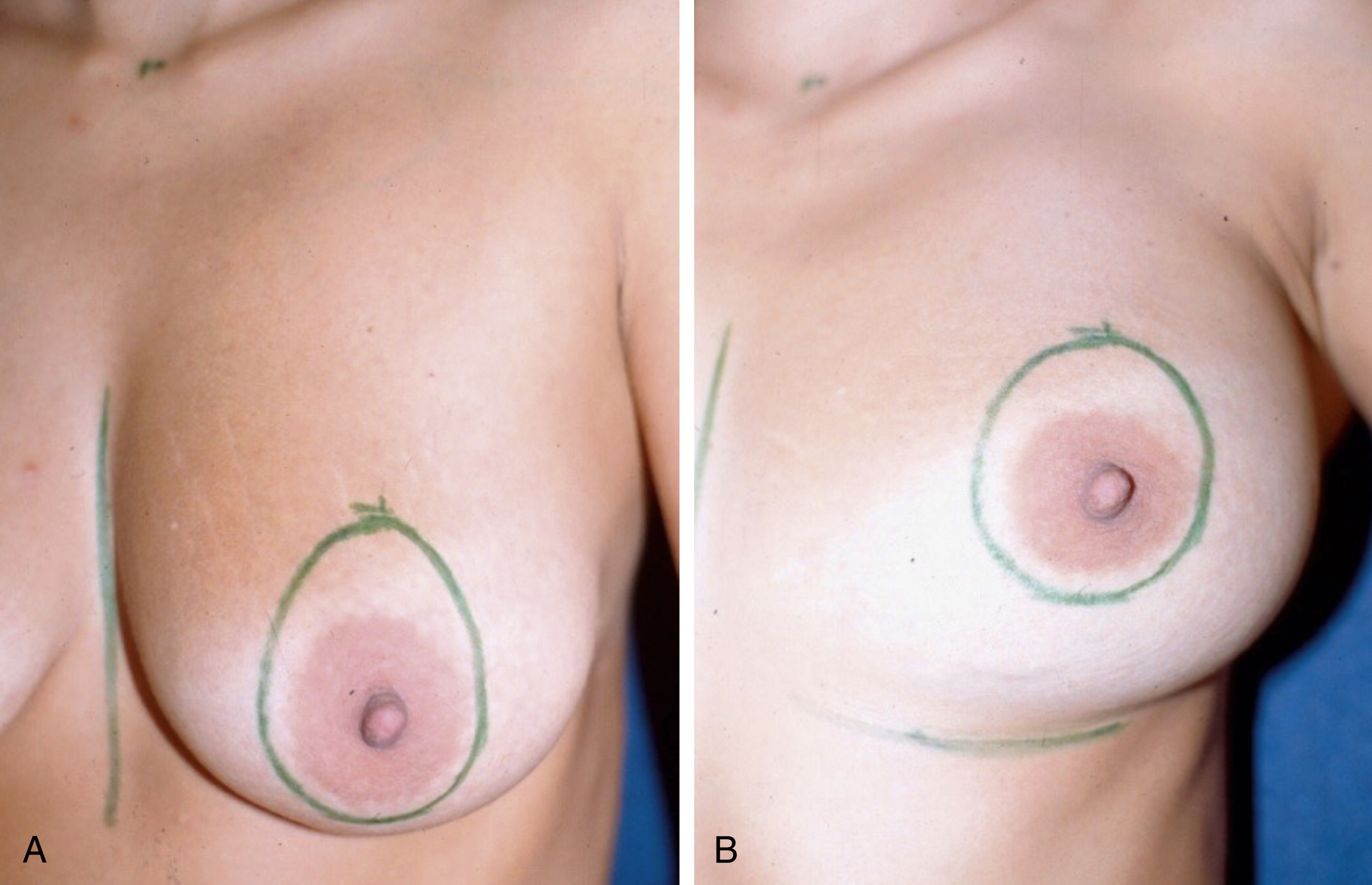
The marking of the periareolar incision should have a teardrop shape with the patient in the standing position, with the longest axis in the vertical direction (A–B) because of gravity ( Fig. 13.3A ) and a more circular shape with the patient in the supine position (see Fig. 13.3B ).
Surgical Procedure
The technique used in periareolar mammoplasty or mastopexy is characterized by the independent treatment of the mammary gland and skin envelope. The technique can be described in 7 steps.
Step 1: De-epithelialization of the Teardrop-Shaped Area
The surgical procedure begins with the de-epithelialization of the previously marked teardrop-shaped area, creating a ring of dermal tissue around the NAC.
Step 2: Flap Undermining
Flap incision and sharp undermining start at the teardrop-shaped area outline. The undermining procedure is performed using different techniques ( Fig. 13.4 ).
Initially, a bevel incision is made on the upper edge of the flap with a progressive increase in flap thickness as it approaches the pectoral fascia. The purpose of this procedure is to increase the fullness of the upper pole of the breast after elevation of the previously reshaped breast mound.
The inner edge of the flap is undermined with a uniform thickness of about 0.5 cm. The undermining is extended to approximately 2 cm from the pectoral fascia. This preserves the intercostal perforators responsible for perfusion of the skin flap and mammary parenchyma.
The undermining of the lower edge also has a uniform thickness of 0.5 cm, extending to the IMF, which must be entirely preserved.
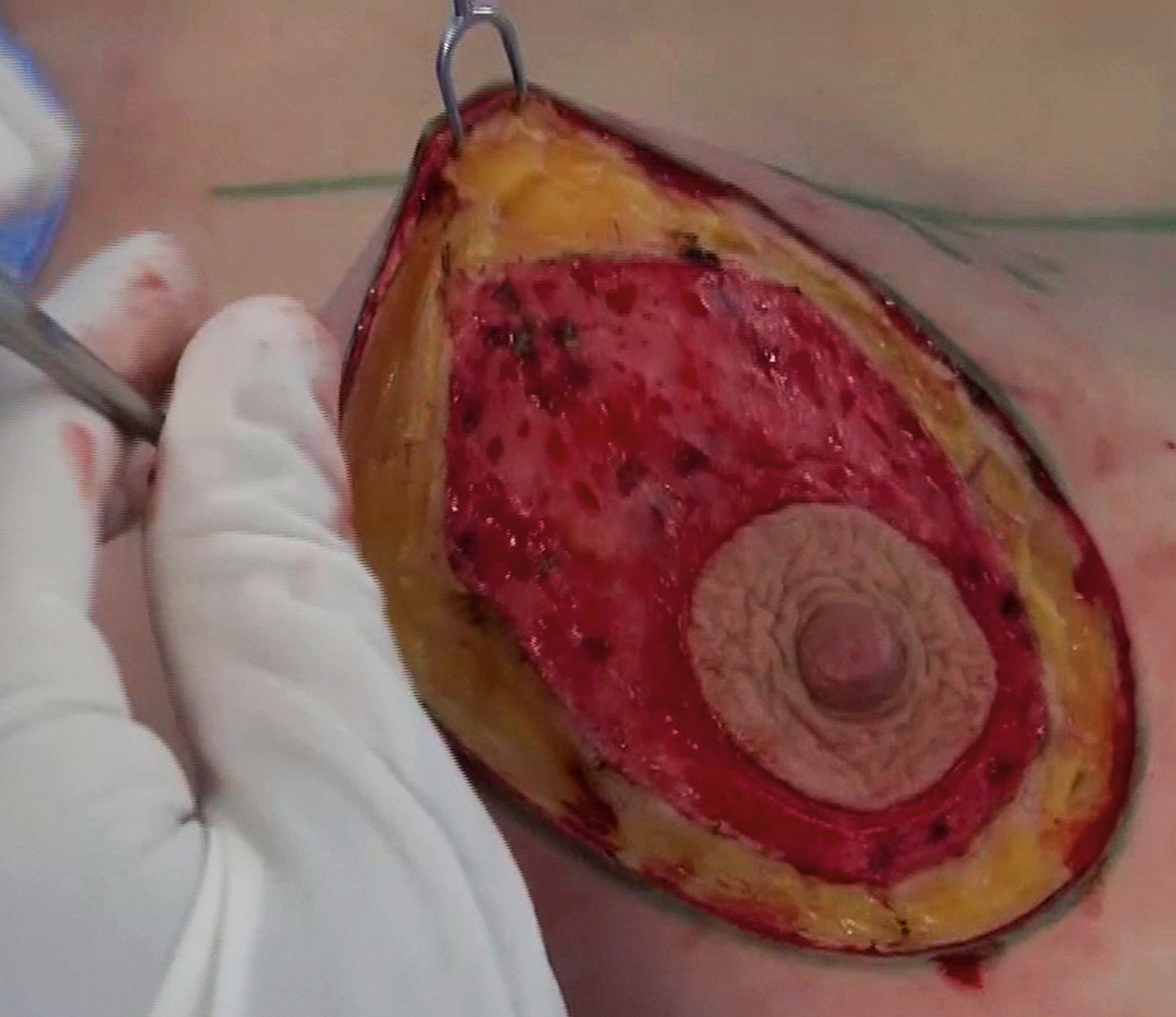
The outer edge of the flap is undermined following the same criteria of uniformity of the inner and lower edges. The sharp undermining is limited by the transition from the breast border to the pectoral fascia, completing the circumferential dissection of the breast ( Fig. 13.5 ).