Mandible Implants
Michael J. Yaremchuk
Dev Vibhakar
Erez Dayan
DEFINITION
Patients with three types of skeletal morphology can benefit from implant augmentation of the mandibular body, angle, and ramus. These skeletal morphologies include those with:
Normal dimensions. Most patients who desire mandible augmentation have lower face horizontal dimensions within normal range. These patients either desire a wider lower face (increased bigonial distance) or desire more definition and angularity to the mandibular border.1
Skeletal deficiency. Approximately 5% of the population in the United States has skeletal mandibular deficiency leading to a class II occlusal problem. Most of these patients can have their dental relationships corrected by orthodontic treatment, which leaves their skeletal contours deficient. These patients can have their mandibular contours improved with implant augmentation.
Surgically altered anatomy. Patients with mandibular deficiency who have had their class II malocclusion corrected by osteotomy and rearrangement remain deficient, but in another way.2 Resultant displeasing postoperative contours include step-offs at the osteotomy sites and malposition of the aesthetically important angle and ramus. Alloplastic implants, particularly those designed and manufactured by computer imaging, can be used to improve contour in these cases.
ANATOMY
All transverse facial dimensions are greater in men than in women with the greatest difference being the bigonial distance.2
Skeletal anatomy
The aesthetically important portions of the mandible are the chin and ramus. The chin determines lower face height and projection in the midline, and the ramus determines lower face width (FIG 1A).
The mental foramen from which the mental nerve exits lies approximately at the interspace between the two premolars and about midway in the height of the dentulous adult mandible (FIG 1B).
Muscular anatomy (FIG 1C)
The four muscles of mastication are predominantly responsible for movement of the mandible and include masseter, temporalis, medial pterygoid, and lateral pterygoid muscles. The only muscles of mastication encountered during mandibular augmentation are the masseter and indirectly the medial pterygoid which together form the pterygomasseteric sling.3
Nerve anatomy (see FIG 1B,C)
Inferior alveolar nerve is a branch of the mandibular nerve (V3). It enters the mandibular canal alongside the inferior alveolar vessels through the mandibular foramen, which is located in the lingual aspect of the ramus approximately halfway between its anterior and posterior borders. It is important to visualize the path of the inferior alveolar nerve when placing screws to immobilize mandibular implants.3 This nerve (now termed the mental nerve) exits at the mental foramen. It provides sensation to the ipsilateral portion of the lower lip.
PATIENT HISTORY AND PHYSICAL FINDINGS
Detailed history should include skeletal trauma, orthodontic therapy, or orthognathic procedures.
Physical examination should explore occlusal relationships, skeletal contour, and relation of the mandible to other facial contours.
Life-size posteroanterior and lateral photographs can be helpful when discussing aesthetic concerns and goals with the patient.
Sample implants and model skulls are useful to demonstrate the application and visual impact of facial implant.
IMAGING
Posteroanterior and lateral cephalograms provide useful data to aid in choosing an implant to best suit the patient.
Three-dimensional computerized tomographic scans and the models obtained from their data can be invaluable in designing implants to correct asymmetries associated with congenital, posttraumatic, or postsurgical deformities (FIG 2A,B).
NONOPERATIVE MANAGEMENT
Soft tissue augmentation in the form of autogenous fat grafts or synthetic fillers can simulate the visual effect of skeletal augmentation to camouflage limited skeletal deficiencies.2,3,4
More aggressive soft tissue augmentation may expand the volume of the soft tissue envelope but at the expense of skeletal definition.2
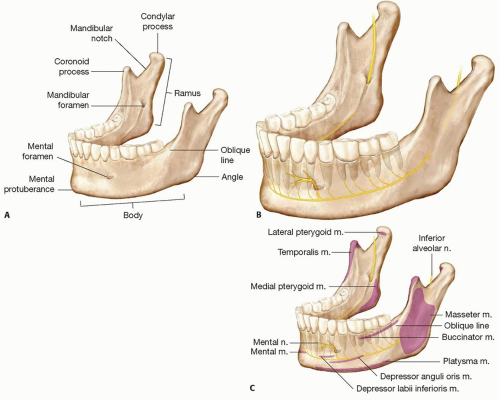 FIG 1 • A. Boney anatomy and relationships of the mandible. B. Relationship of mental foramen to dental anatomy. C. Muscular anatomy of the mandible. |
SURGICAL MANAGEMENT
Preoperative Planning
Patient history, physical examination, possible imaging, and review of patient photographs as well as pictures of others deemed attractive by the patient are all part of the preoperative planning.Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


