(1)
Professor of Plastic Surgery, Director of Diabetic Wound Center, Director of Cell Therapy Laboratory, Korea University College of Medicine and Korea University Guro Hospital, Seoul, Republic of Korea (South Korea)
Abstract
In this chapter, the author attempts to help readers understand the overall treatment of chronic wounds by describing a diabetic foot, one of representative chronic wounds. An accurate understanding of a diabetic foot would also be of great help for the treatment of other types of chronic wounds. In chronic wounds, wound healing cannot often be achieved successfully because of the involvement of multiple factors. Since the clinical characteristics of diabetic feet are very diverse and diabetic patients display a variety of diabetic complications, it is probable that they present all the characteristics of other chronic wounds. There are four representative factors that make it difficult to treat patients with diabetic ulcers. These four factors are termed VIPS. VIPS is the author’s handy treatment tool. The letters stand for vascularity, infection, pressure injury, and source of healing (cell function for wound healing). The management of ischemia and pressure injury is described in this chapter. The management of infection and source of healing are briefly outlined here, and more details will be described in the following chapters.
Keywords
Chronic woundDiabetic ulcerMajor amputationIschemiaWhy Is Diabetic Ulcer Focused On?
Many wound specialists dedicate themselves to conducting studies about diabetic foot ulcers although there are various types of chronic wounds including pressure ulcers, lower leg ulcers (arterial or venous ulcer), and radiation ulcers. Why is understanding a diabetic foot ulcer important? It can be explained with two reasons.
First, there are a great number of diabetic patients, and the number is increasing even at present. According to the World Health Organization (WHO), approximately 5–10 % of adult patients are diabetic. Even in developed countries including the USA, where it has been known to have the most well-managed diabetic patients, approximately 15–25 % of diabetic patients develop diabetic foot (diabetic foot ulcers, diabetic wounds, or diabetic ulcers). Besides, 20 % of patients who are hospitalized due to diabetes have diabetic feet. It is also known that diabetic feet account for 50 % of the total cases of nontraumatic lower limb amputation. If we calculate the rate of patients who have their feet or toes amputated due to diabetic feet, it would be one patient per approximately 30 s worldwide.
Second, another reason that the diabetic foot has been of interest is that its pathophysiology, diagnosis, and treatment are not simple but rather complex. Pressure ulcers occur due to pressure injury, venous or arterial ulcers occur due to abnormalities of blood vessels, and radiation ulcers occur due to the radiation injury. That is, other types of chronic wounds have a definite etiology to some extent. It is therefore relatively easy to decide on the strategy for the diagnosis and treatment of the wounds. Since the clinical characteristics of diabetic feet are very diverse, it is not easy to identify the causes for the lack of wound healing. Diabetic patients display a variety of diabetic complications. It is therefore probable that they may present all the characteristics of chronic wound described above. It would therefore be imperative that other types of chronic wounds be completely understood, which is essential for successful treatment of patients with diabetic feet. This can be compared to the principle that we should have background information about the multiplication or equations to differentiate or integrate functions, although the academic field called the mathematics caters for a variety of areas ranging from addition to multiplication, the first and second degree equations to differentiation or integration.
Why Does Diabetic Ulcer Get into Trouble?
In cases of diabetic foot ulcers, wound healing cannot often be achieved successfully because of the involvement of multiple factors. Diabetic ulcers show different characteristics depending on the patient. Application of only one method may result in solutions that may not match the patient’s specific requirements. It is therefore imperative that the most problematic matter should be identified according to each patient. Favorable treatment outcomes can be obtained so long as patients receive patient-customized treatments.
The treatment of diabetic foot is not simple. In comparison with other types of wounds, the treatment principle and methods are clearly different. Let us look at an example. Since there is a difference in the treatment principle between adults and children, the corresponding clinical areas are divided into the department of internal medicine and that of pediatrics. If there is no difference in the treatment principle, it would also be acceptable to administer the same drugs to children by simply lowering the dose applied to adults. Since this is not applicable, an independent specialty field called the department of pediatrics is needed. Likewise, there should be differences in the diagnostic and treatment methods between diabetic wounds and general wounds.
There are four representative factors that make it difficult to treat patients with diabetic ulcers. These four factors are termed VIPS. VIPS is the author’s handy treatment tool. The letters stand for vascularity, infection, pressure injury, and source of healing (cell function for wound healing). The term, “VIP,” has already been introduced in several literatures. Cases with acceptable blood circulation, no infection, and avoidable pressure are just cases in which the basic conditions are prepared for wound healing. If the wound is successfully closed, the cells around the wound should migrate, proliferate, release extracellular matrices, and thereby restore the defects. It is therefore impossible that successful wound healing occurs in cases in which there is a severe impairment in the functions of the key cells for wound healing. The letter “S” was therefore added by the author. The mnemonic represents both the elements of treatment and the order in which they should be carried out.
In the first part of this chapter, the author attempts to briefly outline the problems and considerations for the treatment of diabetic foot (VIPS). Later in this chapter, details on the management of ischemia are described. Details on the management of infection and source of healing will be described in the following chapters.
Factors Contributing Delayed Healing
Vascularity
Diabetic patients are often accompanied by atherosclerosis in the blood vessels. The blood vessels undergoing atherosclerosis are characterized by narrowing of the vascular lumen due to the deposition of debris such as cholesterol, plaque, and blood clots on the vessel wall. This eventually leads to the insufficiency of the intravascular space where blood circulates. In severe cases, blood vessels can be completely occluded (Figs. 6.1 and 6.2). In cases of blood vessels with smaller-sized lumens, vascular occlusion might occur due to circulating blood clots following detachment from the walls of large-sized vessels. Due to the insufficiency of blood supply, the cells around the wound are given insufficient oxygen or other nutrients that are essential for cell activity. Therefore, vasculoplasty is commonly needed for wound healing in diabetic patients.

Fig. 6.1
Occlusion of the arteries distributed in the ankle joint due to atherosclerosis and blood debris in patients with diabetic feet. (A, B) Blood vessels are visualized even on plain X-ray due to calcification of the debris in the blood vessels (arrows). (C) Gross finding of the occluded vessel. (D) Close-up view
Fig. 6.2
Examples of diabetic feet caused by ischemia
Infection
In cases of wound infections, oxygen or nutrients that normal skin cells should use in the wound healing process are deprived by bacteria. Toxins released by these bacteria degrade normal tissue or regenerated proteins. Unless a complete cure of the infections is achieved, wound healing cannot be achieved. Since the activities of inflammatory cells are generally attenuated due to diabetes, wound infection of diabetic foot usually spreads fast particularly in cases with poor vascularity (Fig. 6.3).

Fig. 6.3
Wound infection of diabetic feet usually spreads fast particularly in cases with poor vascularity
There is a great difference in the diagnosis of infection in patients with diabetic feet from general types of wounds. In cases of general wounds, a diagnosis of infection can easily be made based on the symptoms and physical examination. That is, if a pyogenic exudate is released from the wound site or if there are such symptoms as redness, heat, swelling, and pain, this wound would be under the suspicion of infection. According to the guidelines of Infectious Diseases Society of America (IDSA), in cases with the presence of pyogenic exudate, a diagnosis of wound infection is absolutely made. In cases in which more than two symptoms or signs among redness, heat, swelling, and pain are present, a diagnosis of wound infection can be also made.
However, the abovementioned diagnostic criteria may not be applicable to patients with diabetic feet. The reasons for the emergence of the inflammatory signs at the wound site are that the blood vessels are dilated because myriads of leukocytes should migrate to the wound site to defend against bacteria following recognition of bacterial invasion within the body but also because immunological molecules should be released outside the tissue. The symptoms, heat and redness, occur due to vasodilation. With migration of leukocytes, various molecules and water from the blood vessels leak out to the interstitial space of the tissue, resulting in swelling. Due to the changes in the pH levels in the interstitial space created by the phagocytic activity of macrophages, pain is generated. That is, a diagnosis of infection of general wound can be indirectly made based on the defensive inflammatory responses of the human body against bacterial invasion. In many diabetic patients, however, there is a lower degree of recognition of bacterial invasion due to the immunocompromised status or poor systemic profile. Moreover, these patients cannot have an appropriate defense mechanism against such bacterial invasion.
Therefore, making an appropriate diagnosis of infection or critical colonization in diabetic ulcers can be challenging because diabetic patients may be less likely to demonstrate evidence of infection. White blood cell (WBC) counts are often within the normal range even if there is a definite presence of wound infection. Of patients with severe diabetic feet who concurrently have osteomyelitis, 54 % have been reported to have normal WBC counts. It is therefore mandatory to make a diagnosis of infection based on more direct and objective data in patients with diabetic ulcers, such as tissue cultures. If a wound is considered clean simply based on no inflammatory findings and normal WBC count, successful wound healing may not be achieved.
There are also differences in the strains of pathogenic bacteria between infections of diabetic foot ulcers and general types of ulcers. In diabetic wounds, polymicrobial infections are very common, and anaerobic bacteria are commonly involved. According to reports, more than two bacterial strains are involved in 84 % of total cases of infections of diabetic foot ulcer, and anaerobic bacteria were simultaneously identified from 48 % of total cases. If treatments are simply made using antibiotics that are used for general wounds without making an accurate diagnosis, bacteria would become resistant to the drugs. In addition, deep tissue infections including osteomyelitis are common.
Therefore, a complete cure of infection can be achieved by identifying the exact pathogenic bacteria and the depth of infection.
Pressure
In patients with diabetes, functional abnormalities occur in the nervous system with variability in the severity or symptoms. Neuropathy is present in more than 80 % of diabetic foot patients. Due to the degeneration of the motor nerve, there would be changes in the foot arches resulting in deformity to the shape of the foot and toes (Fig. 6.4). Because of this, pressure is exerted to some parts of the foot during gait. Accordingly, this leads to the progression of skin necrosis. Moreover, due to the degeneration of the sensory nerve, sensory functions are also impaired. This leads to the possibility that the pressure injury on the foot due to gait or shoes cannot be detected as earliest as possible but diagnosed only when skin necrosis has already far advanced. In many cases, patients sweat less because the functions of the autonomic nervous system are also impaired. The skin on the foot is cracked, and bacteria invade the gaps between the cracked skin. This may eventually lead to the occurrence of infection.

Fig. 6.4
Pressure injuries caused by changes in the toe shape
Fibrosis and hardening of soft tissue of the foot can also cause pressure injury. Diabetes changes structure of collagen fibers and therefore causes limited range of motion in the ankle joint. In severe cases, calcified tendons or joint capsules are observed (Figs. 6.5 and 6.6). Stiffness of the ankle joint aggravates pressure injury. In particular, an ischemic foot is extremely sensitive to pressure injury (Fig. 6.7).
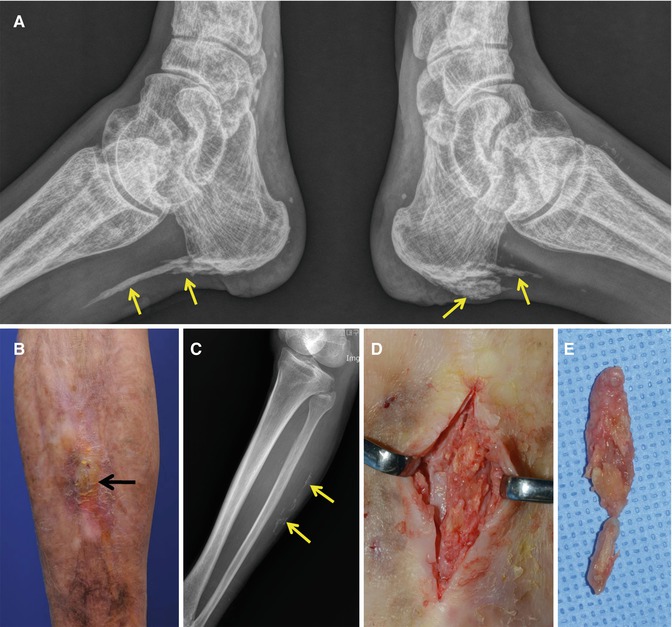


Fig. 6.5
(A) Calcified Achilles tendons (arrows). (B–D) Calcified soft tissue (arrows). (E) Resection of the calcified lesion
Fig. 6.6
Limited motion of the ankle joint by calcification of the joint capsule (arrows)
Fig. 6.7
An ischemic foot is extremely sensitive to pressure injury. In this case, necrosis of the distal forefoot area is mainly caused by ischemia, but the heel is injured mainly by pressure
One of the main precautions when managing patients with diabetes is to be aware of possible foot trauma or undetected wounds. Diabetic patients have a high risk of sensory loss and the resulting loss of pain sensation. It is important to educate patients with foot care guidelines and to provide them appropriate foot wear (Figs. 6.8, 6.9, 6.10, 6.11, and 6.12). The goal is to off-load pressure on the ulcer. Off-loading interventions include therapeutic footwear, custom orthotics, walking casts, and prophylactic surgery.
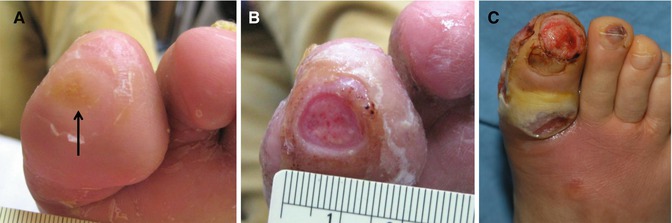



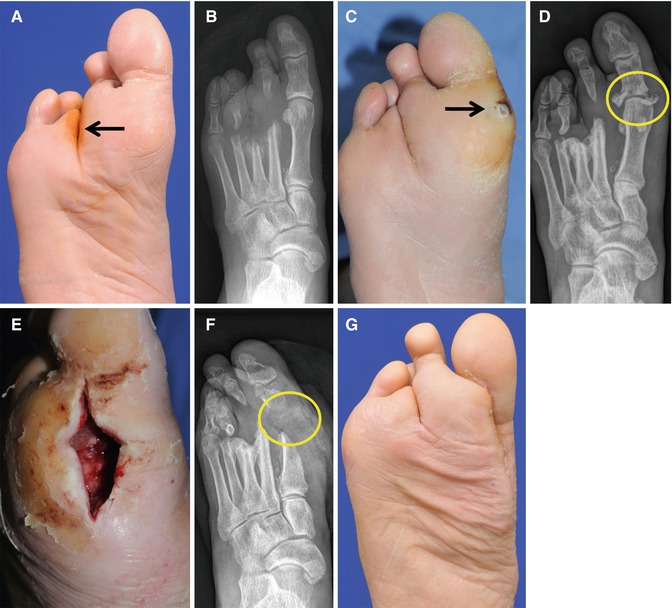
Fig. 6.8
(A) When an abnormal focus of pressure is coupled with lack of sensation, a pressure injury develops (an arrow). (B) If the injury is not properly managed, the injured area eventually breaks open into an ulcer. (C) The ulcer can become infected
Fig. 6.9
Ulcers caused by pressure injuries over the areas of weight bearing (arrows)
Fig. 6.10
Ulcers caused by pressure injuries over the areas in contact with shoes
Fig. 6.11
It is important to educate the patients in foot care guidelines. (A–C) A large, infected plantar ulcer has been successfully treated. (D) One month after the healing, new pre-ulcerative lesions (arrows) developed by the indifference to the pressure off-loading
Fig. 6.12
(A, B) A plantar ulcer previously healed successfully (an arrow). (C, D) After 6 months, a new lesion was developed (an arrow) due to pressure injury. Even though the wound did not show evidence of infection, deep tissue infection including osteomyelitis was demonstrated in a plain radiograph (a circle). (E, F) The infected tissues were surgically debrided (a circle). (G) A view after healing
Therapeutic Footwear
Patients with recurring ulcers and severe foot deformities can greatly benefit from a custom-molded shoe. The common design features include soft, breathable leather that conforms to foot deformities, high tops for ankle stability, rocker soles and bottoms for pressure and pain relief, a toe box with extra depth and width to accommodate deformities, such as clawed toes and hallux valgus, and flared lateral soles for stability.
Custom Orthotics
Custom orthotics are shoe inserts that serve various functions based on the patient’s needs. In general, custom orthotics relieve pressure, reduce shearing and friction, cushion the foot against shock, and accommodate foot deformities.
Healing Sandals
Half-shoes, wedges, and healing sandals are all removable options that can be used to protect and support the feet. They can be removed for wound care/inspection and bathing. Patients must be counseled on the importance of adherence to wearing appropriate shoes.
Walking Casts
Walking casts range from total contact casts to splints and walkers. The use of total contact casting reduces plantar pressures, assists with edema control, reduces shearing forces, protect from trauma and microorganisms, and assists with increasing patient adherence. Total contact casts are contraindicated for those with gangrene, osteomyelitis, fluctuating edema, infection, and foot ischemia. Patients with fragile skin may benefit from a walking splint.
Author’s Methods
The author has used a variety of methods to relieve pressures on the wound depending on the location of the wound (Figs. 6.13, 6.14, and 6.15).
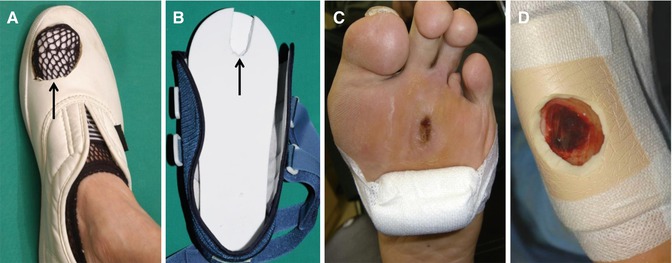

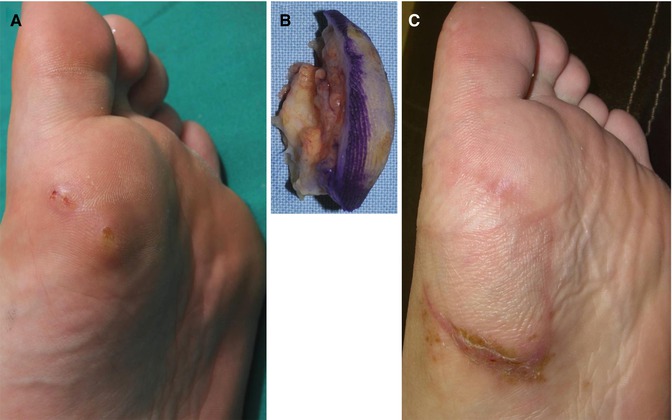
Fig. 6.13
The author’s methods for pressure off-loading. (A, B) Making holes in shoes (arrows). (C, D) Attaching cushion pads around the wounds
Fig. 6.14
Effect of proper off-loading on wound healing. (A) A ulcer on the great toe. (B) After 2 weeks, the ulcer size was significantly reduced. However, plantar portion of the wound, a weight-bearing site, did not improve. (C, D) After applying a cushion pad, the plantar portion of the wound also began to show signs of wound healing
Fig. 6.15
In a selected patient who has favorable blood supply to the foot, the pressure injury can be treated by a local flap coverage. (A) A pressure injury on the 1st metatarsophalangeal joint area. (B) An excised scar tissue. (C) The defect was covered by a local flap transferred from non-weight-bearing medial plantar area
Source of Healing (Cell Function)
For successful wound healing, the key cells for the wound healing including macrophages, fibroblasts, and keratinocytes should have satisfactory activities. These cells release various cytokines and thereby regulate the wound healing process including the inflammatory response, migration and proliferation of cells, synthesis of extracellular matrices, and angiogenesis. In diabetic patients, however, cells have notably decreased mitotic activity compared with normal healthy controls. Besides, there is an insufficient degree of synthesis of extracellular matrices. Therefore, production of proteins including growth factors that are essential for wound healing cannot be well achieved. Conversely, secretion of matrix metalloproteinase which destroys tissue proteins becomes activated. Because of this, there are often cases in which the wound healing process is interfered. The degree of cell migration is also decreased. Therefore, the wound remains open without being cured for long periods of time. This eventually leads to infections. It would therefore be mandatory to activate these cells during treatment (Fig. 6.16).
Fig. 6.16
Activation of diabetic fibroblasts by cell therapy. Human diabetic fibroblasts from the same patient were cultured with or without stromal vascular fraction (SVF) cells obtained from adipose tissue. (A) Control group fibroblasts. (B) SVF cell treated fibroblasts
In addition, various factors for wound healing including albumin, minerals, and various vitamins, all of which are essential for wound healing, would become depleted because of the presence of diabetes and poor systemic condition (details in Chap. 11). If wounds are only topically treated without replenishing the deficient factors, it is likely that the wounds will not be optimally repaired.
Risk Factors for Major Amputation
Diabetic foot lesions are significant health and socioeconomic problems with adverse effects on the quality of life. Diabetic foot is the main cause of nontraumatic lower extremity amputation. For the purpose of preventing serious complications like generalized infection or septic condition, diabetic foot ulcer has been commonly treated with minor or major amputation. Minor amputations include partial toe amputation, complete toe amputation, partial or full ray resection, and proximal foot amputation (transmetatarsal, Lisfranc’s, Chopart’s, and Symes amputations). Below-the-knee and above-the-knee amputations are considered major amputations.
Major amputations are associated with high rates of postoperative mortality and morbidity since they have been associated with increased cardiovascular demand in a subset of patients who already have an increased prevalence of cardiovascular disease. A retrospective study by Aulivola et al. revealed a mortality rate of 8.6 % at 30 days and overall survival of 69.7 % at 1 year and 34.7 % at 5 years after major amputation.
Several risk factors for major amputation among the patients with diabetes have been cited in the literature, including age, male sex, size or depth of ulcer, foot infection, hypertension, peripheral arterial disease, neuropathy, nephropathy, dialysis, poor glycemic control, white blood cell count, and lipid abnormalities. However, there are inconsistencies in the results of the studies. Since previous studies were mainly conducted on a multicenter basis, management protocols for diabetic foot ulcers might vary widely according to hospitals. So far, there has been no large-scale study in patients who were treated using the identical management protocol for this subject.
The author has performed a clinical study to determine the risk factors for major amputation in patients with diabetic foot ulcers who received standard treatment at a referral center for diabetic foot ulcer. This study included 837 diabetic patients who were admitted to the author’s Diabetic Wound Center. Among them, ulcers in 809 patients (96.7 %) healed without major amputation, and those in 28 patients (3.3 %) healed with major amputation. Data of 88 potential risk factors including demographics, ulcer condition, vascularity, bioburden, neurology, and serology were collected from patients in the two groups and compared between them. Among the 88 potential risk factors, statistically significant differences between the two groups were observed in 26 risk factors. In the univariate analysis and the stepwise multiple logistic analysis, 6 risk factors remained statistically significant. The risk factors for major amputation in diabetic foot patients were bony invasion, dialysis, gastrointestinal disorder, hind foot location, low level of hemoglobin, and elevated fasting blood sugar level.
Management of Ischemia
Adequate tissue oxygenation is an essential factor in diabetic foot management. The importance of blood flow and oxygen delivery to a wound bed cannot be overstated.
Diagnosis of Arterial Insufficiency
It is critical that the presence and severity of circulatory compromise are determined before making a prognosis for wound healing and to develop an appropriate plan of care (Figs. 6.17 and 6.18). There are a variety of tests and measures available to assess for arterial insufficiency.
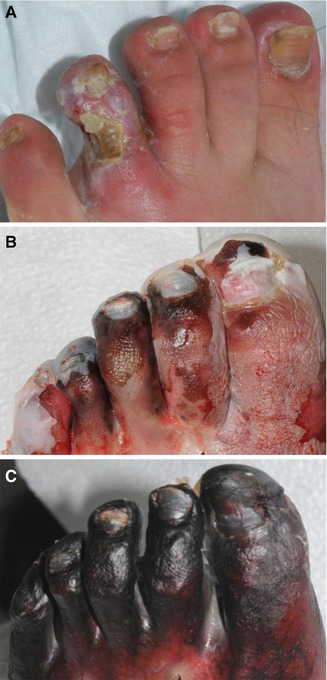
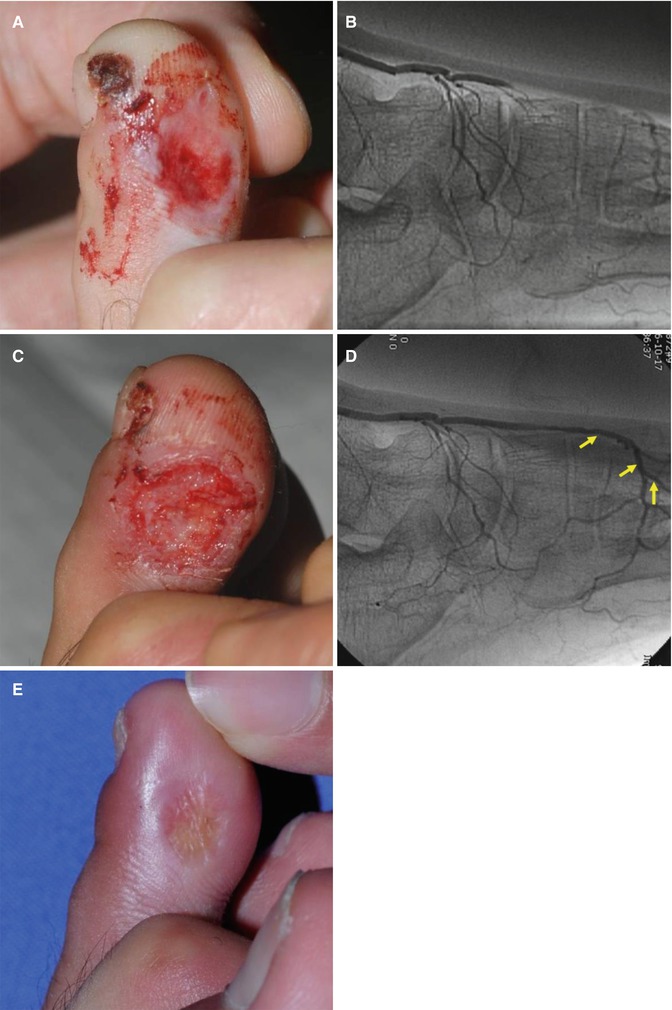
Fig. 6.17
Topical wound care without determining the presence of circulatory compromise may result in the loss of the entire foot in diabetic patients. (A) A diabetic ulcer on the 4th toe. (B) One week later. (C) Two weeks later
Fig. 6.18
Treatment with an appropriate plan of care is essential to diabetic patients for successful healing. After identifying occlusion of the dorsalis pedis artery (A, B), angioplasty (arrows) was preceded before topical wound care (C, D). (E) Complete healing was achieved
Capillary Refill
The capillary refill test is a reliable indicator of surface arterial blood flow. It is measured by pushing against the lesion with enough pressure to blanch the skin and holding for five seconds.
Normal capillary refill time is less than 3 s. Patients with arterial insufficiency will have delayed capillary refill (Fig. 6.19).

Fig. 6.19
Capillary refill test
Rubber of Dependency
Rubber of dependency is a test used for indirectly assessing arterial flow in the lower extremities.
With patient in the supine position, the color of the plantar aspect of the foot is noted. The lower extremity is elevated between 45° and 60° for one, minute and the color of the foot is noted again. Patients with normal arterial flow will exhibit little or no color change. However, in patients with arterial insufficiency, the skin of the affected extremity will be pale.
The leg returns to the surface, and the time for return of the original color is noted. Those with normal arterial supply will have the color return to normal color in 15–20 s.
Venous Filling Time
Prolonged venous filling time is predictive of arterial insufficiency.
To perform this test, first ask the patient to lie supine and note the superficial veins on the dorsum of the foot. After this, elevate the lower extremity to approximately 60° for one minute or until veins are drained by gravity. Next, place the limb in the dependent position and record the time it takes for veins to refill.
Normal venous filling time is 5–15 s; >20 s indicates arterial insufficiency.
Pulses
It is important that peripheral pulses should be checked in both the involved and uninvolved extremities. Pulses should be taken with patient in the supine position. Pulses of the femoral, popliteal, dorsalis pedis, and posterior tibial arteries are usually assessed.
The bifurcation of the common femoral artery into the superficial and deep femoral arteries is the most common site of occlusion. An absence of palpable pulse should be followed up with more sensitive testing.
Doppler Ultrasound
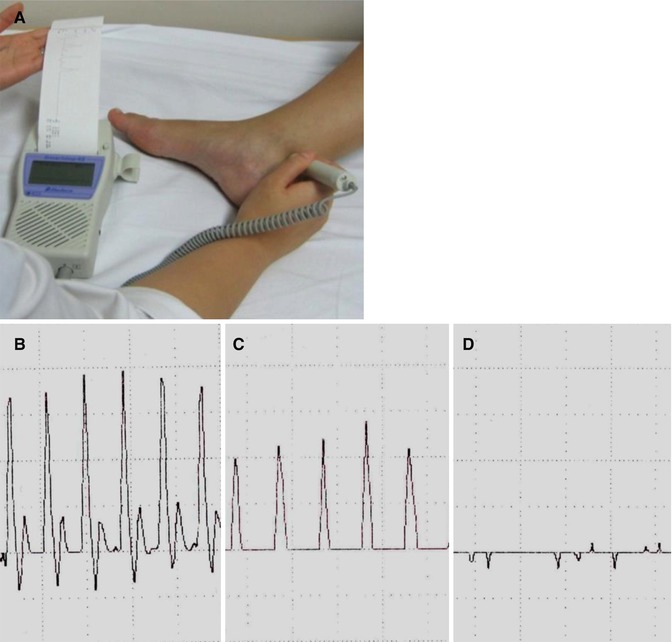
When peripheral pulses are not easily palpable, Doppler ultrasound can be used to further assess arterial patency. Among the many methods currently used for predicting the healing potential in diabetic foot patients, Doppler probing is noninvasive, probably the easiest to perform, and most widely used.
Doppler probing utilizes the Doppler effect of ultrasound waves (the wavelength and frequency of waves reflected on moving blood flow changes, unlike the waves that are reflected on stationary objects) to evaluate blood flow in vessels. Doppler signals are sensitive enough to detect blood flow inside vessels in which pulsation is not palpable, and audible signals emitted from Doppler probes sufficiently convey information on the patency of vessels (Fig. 6.20).