(1)
Professor of Plastic Surgery, Director of Diabetic Wound Center, Director of Cell Therapy Laboratory, Korea University College of Medicine and Korea University Guro Hospital, Seoul, Republic of Korea (South Korea)
Abstract
Deep tissue injuries have many functional and cosmetic features that pose limits on available treatment options, especially when bones, joints, or tendons are exposed. Such instances have been treated using various types of flaps, including local, distant, island, and free flaps. However, conventional flaps may be inappropriate in some cases due to limitations in size, arc of rotation, flap bulkiness, sacrifice of an artery, long operation time, need for microsurgery techniques, etc. Possible promising alternatives for management of such scenarios are arterial and venous island flaps. Unlike conventional axial pattern flaps, they rely on the arterial or venous system alone for flap perfusion. The atypical flaps have many advantages over more conventional flaps. There is no need for a microsurgical procedure and donor site morbidity is minimal. These relatively simple and time-saving procedures are done in one stage, avoid uncomfortable immobilization, and shorten the period of hospital care. Further advantages include excellent sensory restoration is possible and cosmetic results are acceptable. These atypical artery- or vein-only island flaps are particularly versatile in hand coverage. The aim of this chapter is to report the usefulness and postoperative results of arterial and venous island flaps for coverage of deep tissue defects.
Keywords
Island flapArterial flapVenous flapArterial Island Flap
Distally based arterial island flap or reverse digital artery island flap is a useful option for a tissue defect on the areas of the fingertips. Fingertip injuries represent the most common type of injuries seen in the upper extremity. Their management is functionally and aesthetically important but at the same time very controversial. The goals of fingertip treatment are preservation of functional length and sensibility, prevention of symptomatic neuromas and of adjacent joint contracture, and minimization of aesthetic deformity.
The distally based arterial island flap in the finger was first described by Weeks and Wray in 1973; since then, several authors have introduced modifications to this distally based arterial island flap. The reverse digital artery flap has many advantages over more conventional flaps. This relatively simple and time-saving procedure is done in one stage, maintains the finger length with sufficient soft tissue padding, provides thin and hairless skin, avoids uncomfortable immobilization, and shortens the period of hospital care. Further advantages include excellent sensory restoration is possible, donor site scar can be hidden, cosmetic results are acceptable, and the flap can be used in multiple fingertip amputation cases.
Surgical Technique
The flap is designed in a round or stellate shape to avoid scar contracture on the ulnar or radial side of the proximal phalanx of the finger with a digital artery as the central axis according to the size and shape; however, the least-used side of the finger is chosen if possible. In extended flaps, the dorsal skin over the metacarpophalangeal joint as well as the lateral skin of the proximal phalanx can be included. The author has reviewed the sizes of the flap used, and the length and width of flaps were found to range from 1.6 to 3.2 cm and 1.0 to 2.5 cm, respectively, with a maximum size of 3.2 × 2.5 cm.
The operation is carried out under regional block or general anesthesia. After minimal debridement of the wound, the size and shape of the defect are measured. After pneumatic tourniquet inflation, skin incision is made, and the flap is elevated carefully with the aid of surgical loupe magnification. The digital artery is first identified and then separated from the proper digital nerve to the level of about 5 mm proximal to the distal interphalangeal joint to transfer the flap freely but, at the same time, not to injure the middle transverse digital palmar arch (Figs. 5.1 and 5.2). However, the digital artery may be dissected more distal to the level of distal interphalangeal joint in cases in which there are enough remaining finger pulp to include vascular communications between the radial and ulnar proper digital arteries. The author usually considers the center of the fingerprint as an indicator. If this remains in the recipient site, the digital artery can be dissected more distally. This maneuver enables the flap to move to the very distal part with ease.
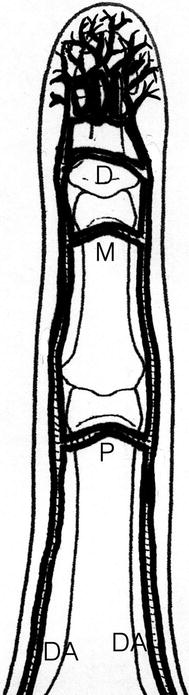
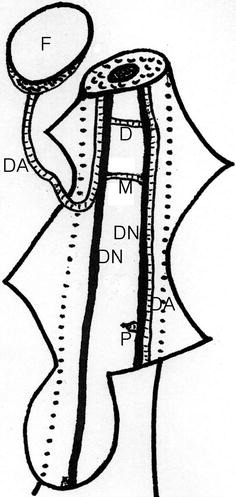
Fig. 5.1
Digital arterial system of a finger. Three transverse digital palmar arches between digital arteries and abundant vascular communications exist in the pulp of a distal phalanx. DA digital artery, P proximal palmar arch, M middle palmar arch, D distal palmar arch
Fig. 5.2
Diagram of the reverse digital artery island flap. The flap is perfused from the opposite side of the proper digital artery through the middle transverse palmar arch and then to the ipsilateral proper digital artery, F reverse digital artery island flap, DA digital artery, DN digital nerve, P divided proximal palmar arch, M middle palmar arch, D distal palmar arch
A generous cuff of subcutaneous tissue is maintained around the vascular pedicle to preserve the tiny perivascular venules. The digital artery at the proximal end of the flap is ligated and divided.
In cases of sensate flaps, the dorsal branch of the digital nerve or the superficial sensory branch of the radial or ulnar nerve attached to the flap is identified and dissected and then microanastomosed to the digital nerve at the defect by the epineural method. However, the author does not employ sensate flaps anymore because the long-term results have not shown a significant difference between sensate and insensate flaps and the inconvenience of additional operating time required for innervated flaps. Sensory recovery in the insensate flap comes from collateral sprouting from adjacent intact nerves and central adapting mechanisms.
The flap is transferred and loosely sutured to the defect, not compressing the pedicle. A skin graft is applied to the donor defect. Postoperatively, the operated hand is elevated, and no anticoagulants are used.
Regarding the venous system, the reverse digital artery flap is drained through the tiny venules and capillaries contained in the perivascular soft tissue.
Clinical Study
One-hundred forty fingers with defects of the distal phalanx were reconstructed by the author using the reverse digital artery flaps. Survival of the flaps was successful in all fingers except for one. In 20 fingers, postoperative congestion developed but spontaneously subsided within 2–3 days in all cases. Postoperative sensory recovery was excellent in all cases. All of the evaluated flaps had the ability to detect light touch, temperature, and sharp stimuli. Regarding scar contracture, no patient required an additional operation for further improvement of the fingertip shape, although a mild irregularity was seen at the flap edge in three of the patients (Figs. 5.3 and 5.4).

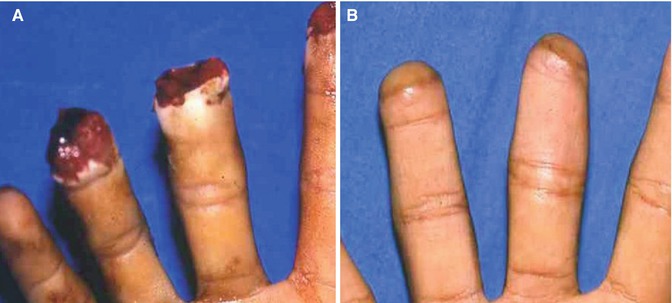
Fig. 5.3
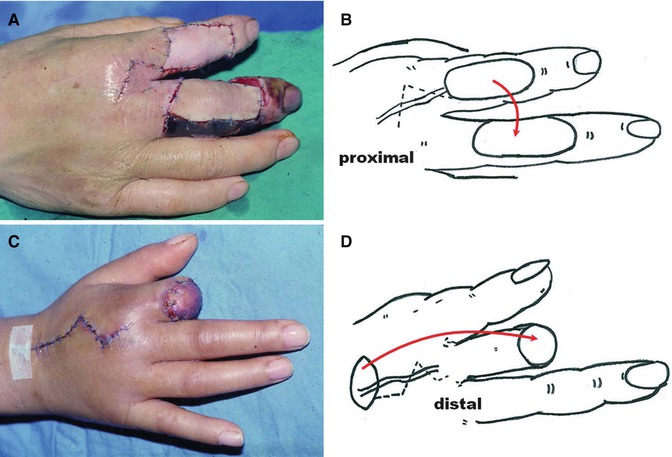
(A) Preoperative design of an insensate reverse digital artery flap. (B) Immediate postoperative view after flap transfer by extensive dissection of the digital artery to the level of the distal interphalangeal joint. (C–E) One year after the operation. Active full range of motion is demonstrated
Fig. 5.4
A 21-year-old man’s right middle and ring finger pulps were cut. (A) Preoperative view. (B) Reconstructed fingertips 2.5 years following reverse digital artery flap coverage
Venous Island Flap
Venous island flaps are also useful for wound coverage of the hand. Venous flap is defined as a flap of the skin and subcutaneous tissue that utilizes venous inflow and outflow for its nutrient supply. In the anatomy of the venous system in the hand, valves are directed from distal to proximal and from palmar to dorsal. Although valves do not allow retrograde venous flow, reverse venous blood flow is possible after denervation, the presence of venous blood on either side of the valve, or high proximal venous pressure. Chavoin et al. reported that the superficial and distal veins of the limbs have few valves and dilate easily.
Venous flap perfusion hypotheses include plasmatic imbibitions, pulse pressure in the preserved draining vein, and revascularization from the recipient bed with good blood circulation. Furthermore, some experimental studies have shown that a single proximal vein of a venous flap can provide sufficient flap perfusion and drainage. Sasa et al. reported that venous drainage from a venous flap may be critical because more rapid rearterialization can occur in the presence of venous outflow and venous plexus when the flap enables nutrients and oxygen to reach flap cells by reverse flow, thus, enabling them to survive until rearterialization occurs. Inada et al. and Fukui et al. demonstrated clinically that venous pressure gradients promote successful survival. Another possibility of venous flap survival is that the oxygen content of venous blood in venous flaps is sufficient for flap survival, because only 25–30 % of oxygen in arterial blood is utilized. In addition, fat and skin have low metabolic rates and their metabolic requirements are reduced after the flap is raised. However, the prevalence of necrosis demonstrates that venous island flaps are not intrinsically safe, and thus, some authors have emphasized the importance of the relationship between perivenous areolar tissue and venous flap survival. They reported that “perivenous network” in areolar tissue was important for the perfusion of venous flaps and provided sufficient inflow with good venous drainage, which required venous pedicles be raised with careful dissection to preserve as much perivenous areolar tissue as possible. However, blood supply to the venous island flaps remains controversial, and there is no clinical consensus regarding the mechanism of flap survival. A combination of the abovementioned factors may be the reason for venous flap perfusion.
Venous island flaps of the hand have several advantages. First, there is no need for a microsurgical procedure. Second, there are numerous donor sites with available superficial dorsal veins, which make surgery relatively straightforward. Third, the procedure requires only one stage. Fourth, donor site morbidity is minimal and there is no need to sacrifice any major artery at the donor site. Finally, thin and pliable flaps can be obtained.
Surgical Technique
A tourniquet is applied on an upper arm using a pressure of 100 mmHg, which allows the veins to engorge. Vein distribution is then traced onto the surface of the skin with a marking pen. The pedicle is decided according to the defect site and vein distribution. After completing the design, the tourniquet pressure is increased to 250 mmHg, and the skin is incised in a zigzag fashion from the donor site to the pivot point. Flaps are dissected on the muscle fascia or paratenon and include only the skin, subcutaneous tissue, and attendant veins. After ligating and cutting a venous pedicle at the flap end, a venous pedicle is raised with careful dissection to preserve as much perivenous areolar tissue as possible. The flaps are transferred and inset to cover the defects either through a subcutaneous tunnel or an extended skin incision. Donor sites are repaired directly or with skin grafts (Fig. 5.5).