Chapter 12 Mammaplasty with L-shaped scar
• The Phi ratio 1/1.618 defines breast aesthetics in a three dimensional perspective
• Breast shapes and volume alterations occur accordingly to specific classifications
• The L-shaped scar mammaplasty along with techniques to produce a cone-shaped breast mound is a versatile technique in breast surgery
Introduction
Throughout human evolution the limbic brain systems have been marked out with the attractive features of what is visually beautiful. One mathematical proportion (Phi) has been repeatedly stated to be found in beautiful general forms until the present. “There’s probably a natural connection between the sense of beauty and efficiency that is biologically necessary for individual survival. Phi seems to present single and wonderful properties. It is a quality that for some reason attracts attention, and it is registered in the limbic system such as beauty, harmony and balance”.1 Phi is a universal constant ratio of 1/1.618 (Fig. 12.1).

The Greek philosophers Plato, Aristotle, Pythagoras, and Euclid studied the proportion Phi (1/1.618) known as the Phi ratio and felt that beautiful creations respected certain geometrical laws displaying harmony.2 It is not known when the Phi ratio was first described or applied but it has always existed in the fields of mathematics and physics. Because the Greek sculptor Phidias used that proportion so much, it was called Phi, the Greek letter for the first part of his name. This proportion was also described by Leonardo Fibonacci of Pisa, in his development of mathematical sequences. Leonardo da Vinci called it the “golden proportion” and used it in Vetruvian Man. It has been used in the design of such classic edifices as the Parthenon. Botanists have found it in phylotaxy.3 In the twentieth century there were psychological studies about significant preferences for structures containing the Phi proportion.4
Proportions and Anatomy of the Beautifully Shaped Breast
Shape and Volume
Frontal View
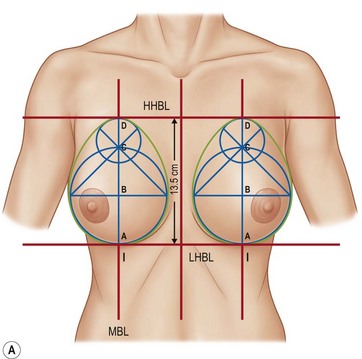
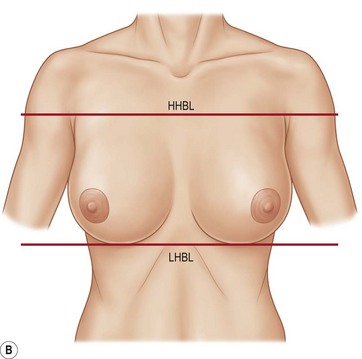
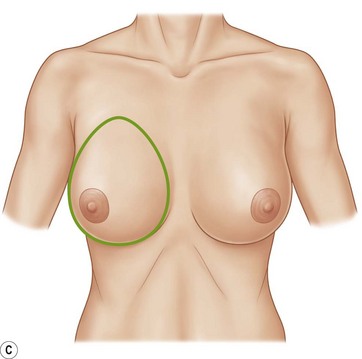
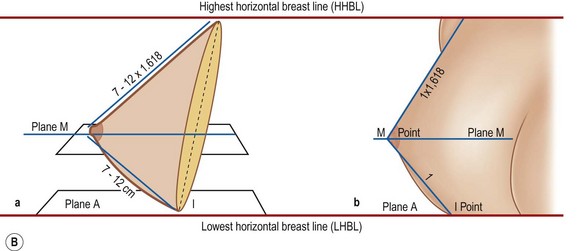
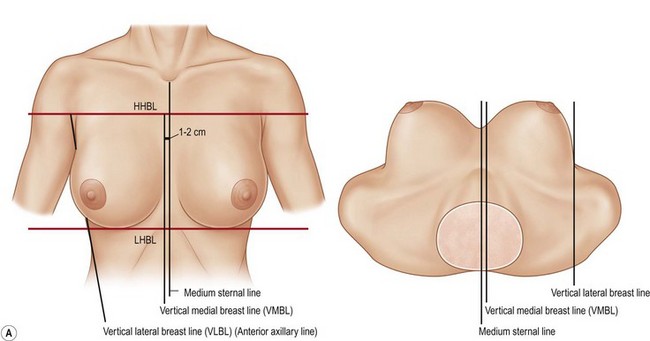
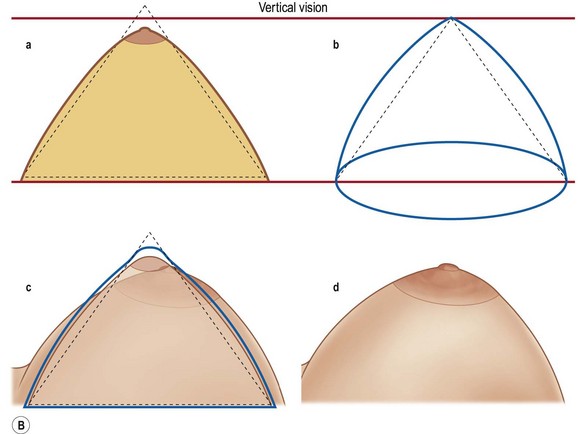
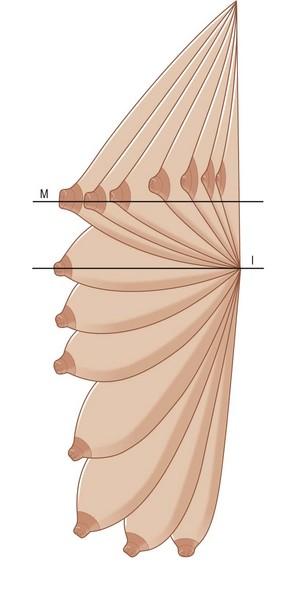
Considering the shape of the breast as an irregular cone, the horizontal diameter is smaller than the vertical in a ratio of 1 to 1.3. This ratio is the consequence of the application of Phi to the vertical axis with the shape of the golden oval (Fig. 12.2A–C). The axis ABCD (Fig. 12.2A). is the breast meridian line (BML) and it is comprised of two other horizontal lines: the lowest horizontal breast line (LHBL), which connects the inframammary sulcus where it meets the breast meridian line (points I); and the highest horizontal breast line (HHBL), which connects the highest point of the two anterior axillary folds. The vertical measure between both lines is a single mark for each patient, determining the vertical extension of the base of the breast. Applying the ratio of 1 to 1.3 to this, the consequential and proportional lateral extension is obtained.
Lateral View
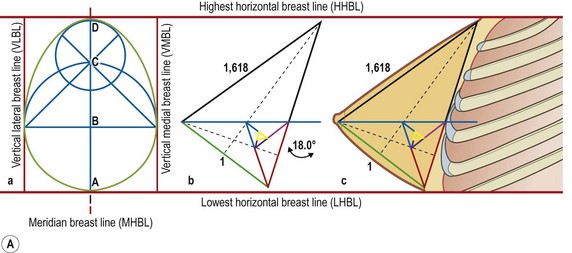
The normal thoracic skeleton in the anterior external costal region has an anatomic inclination of approximately 18° in relation to the vertical axis of the body in the area of the breast implants. When the golden triangle is inclined over this angle in relation to the vertical plane, it will resemble the beautiful breast from the profile (Fig. 12.3A, B).
Vertical View
From the vertical point of view of the individual, when the patient looks at herself from above, the normal, beautiful breast is between two vertical lines: the vertical lateral breast line (VLBL) and the vertical medial breast line (VMBL). The former coincides with the anterior axillary line; the latter is situated 1 to 2 cm laterally to the middle line of the sternum (Fig. 12.4A, B).
Diagnosis of Breast Shapes and Volume Alterations
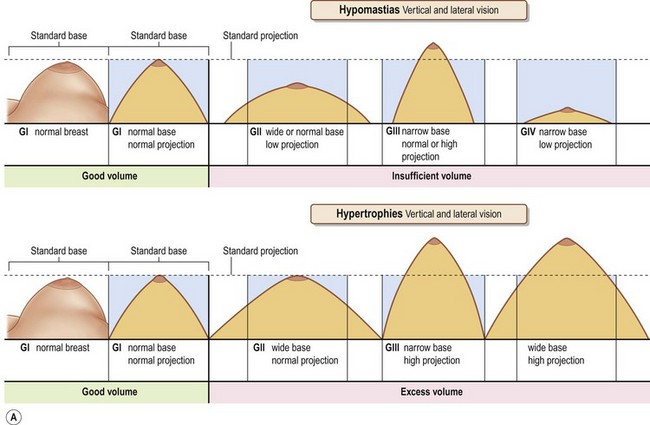
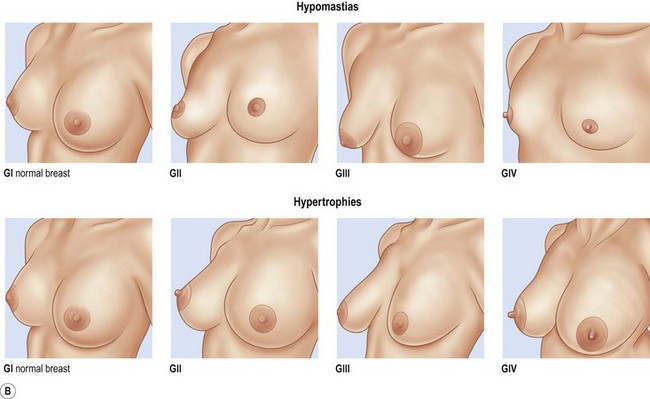
According to the frontal, lateral and vertical views (base and cone projection without ptosis), it is possible to observe the various shapes of the breast and to classify hypomastias and hypertrophies (Fig. 12.5A, B).
Group I: The breast is normal (normomastia). Base, profile and projection fall within the golden ovoid, golden triangle and golden cone, respectively. They fit within the two horizontal lines (HHBL and LHBL) and the two vertical lines (VMBL and VLBL) previously referred to. This is the control group described in “earlier”. The characteristics of Group I are the same for both hypomastia and hypertrophy classifications.
Group II hypomastia: The diameter of the breast base is normal or widened, but without an ideal projection. There is insufficient volume.
Group III hypomastia: This is the opposite of Group II. The projection of the cone is normal or augmented and the diameter of the base is reduced. There is insufficient volume.
Group IV hypomastia: The projection of the cone and its base are diminished or absent. There is insufficient volume. Amastias are included in this group.
Group II hypertrophy: The diameter of the base is widened and the projection is normal. Excess volume is on the increase of the diameter of the base.
Group III hypertrophy: It is the opposite of Group II, the projection of the cone is increased and the base diameter is normal or reduced compared to Group I. The excess volume is in the projection.
Group IV hypertrophies: This is the sum of both Groups I and III, the volume in excess is on the base enlargement and in the projection of the mammary cone.
Flaccidity (Ptosis)
The anteroposterior growth projects the breast into space and subjects it to gravitational forces; progressively the breast falls, except at point I of the inframammary sulcus. This ptosis starts after puberty and continues throughout life (Fig. 12.6).
In lateral view: the thorax is considered to be a vertical plane and the breasts are placed on it. If we observe no ptosis, it is like the initial description, above plane A with no ptosis. The falling breast (where planes A and M coincide) still has no mammary ptosis is still zero (on the breast borderline). The superior upper pole is partially emptied. As the ptosis continues, plane M will exceed down the plane A. Ptosis is installed (Fig. 12.7A).
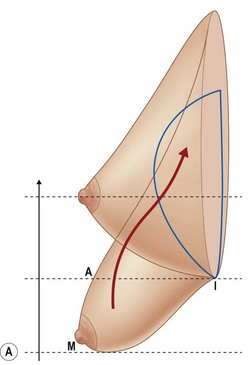
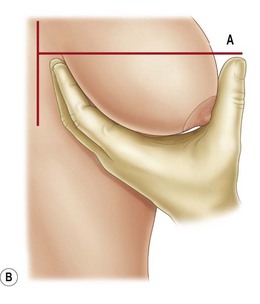
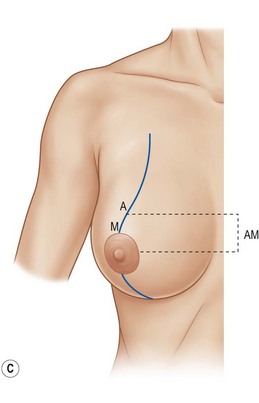
In the frontal view: the vertical diameter is reduced, and the horizontal widened; they have reversed themselves. The upper pole is empty. The distance between points A and M on the meridian that crosses the two planes will quantify the ptosis in centimeters, and consequently the amount of skin to be removed in the mammaplasty. The plane A and point I remain unchanged throughout life. Now with the reversal of the increased diameter of the base, the vertical is smaller and horizontal is greater and the beauty of the breast shape has been lost. In practice, with the patient standing, one can get the mammary meridian, and three points: A, projection of point I over the breast, in plane A (Fig. 12.7B); M, the apex of the mammary cone on the mammary meridian, and I (crossing the meridian with the inframammary sulcus). Point M is not the papilla – it should be, but this may be “ectopic” in relation to the apex of the breast from irregular growth of the mammary cone during puberty.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


