Key Points
- •
Lymphoscintigraphy is an objective and reliable imaging modality for diagnosing lymphedema, categorizing its severity, and guiding appropriate treatment.
- •
The diagnostic utility of lymphoscintigraphy depends upon meticulous technical performance and correct image interpretation.
- •
The main drawback of lymphoscintigraphy is the lack of standardized protocols, making comparisons among the studies difficult.
- •
Several lymphoscintigraphic staging or scoring systems have been proposed, with variable clinical applications. The recently validated Taiwan Lymphoscintigraphy Staging (TLS) system includes the most relevant lymphoscintigraphy findings grouped by severity, providing an easy tool for the diagnosis and severity categorization of lymphatic obstruction.
- •
The Cheng Lymphedema Grading system, combined with additional TLS information, is a promising lymphedema grading system for patient selection regarding surgical treatments.
Disclosures : Ming-Huei Cheng received textbook royalties from Elsevier, Inc.
Introduction
Extremity lymphedema represents a chronic debilitating disease with a high tendency to progress, which may increase physical disability and recurrent cellulitis in the advanced stages without adequate treatment. The progression of lymphedema can lead to significant decreases in overall patient-reported quality of life outcomes, with significant physical and visual discomfort. With the increasing availability of lymphedema treatments and awareness of the problem, early recognition and diagnosis are now possible for reducing the morbidity and for the successful treatment of these patients. Extremity lymphedema is usually diagnosed through history and physical examination. However, diagnosis and severity determination can be a challenge for the physician in an attempt to find and start an effective treatment. A number of imaging modalities can be used to aid in the diagnosis of lymphedema. Lymphoscintigraphy was first introduced in 1950 and has become, for many years, the benchmark procedure for the diagnosis of lymphedema with the ability to visualize the functional status of the lymphatic system. The procedure is minimally invasive, easy to perform, and safe as radiotracers rarely cause an allergic reaction. It involves the injection of a protein or colloid with a radioactive technetium-99m ( 99m Tc)-labeled tracer into the web spaces of the fingers or toes. Then, the radiotracer is taken up by the lymphatic system through the lymphatics, the collectors, and transported to the proximal limb of the inguinal or axillary lymph nodes. This nuclear medicine procedure is able to visualize proximal lymph node uptake, visualize superficial and deep lymphatic vessels, and detect abnormal lymphatic findings. The main limitation of lymphoscintigraphy is the lack of a standardized protocol and the occasional poor image resolution. Hence, making comparisons between lymphoscintigraphic studies in the literature is confounded by the variety of protocols with heterogeneous results and conclusions.
The use of lymphoscintigraphy varies worldwide. Although in some centers, it is performed for almost all patients with suspected lymphedema as a routine part of the diagnosis, in others, it is rarely applied, mainly due to unfamiliarity with the interpretation of this imaging modality.
Several lymphoscintigraphic staging or scoring systems have been proposed in the literature, with variable applications in clinical practice. The recently validated Taiwan Lymphoscintigraphy Staging (TLS) system is correlated with objective clinical findings and has been developed to provide an easy tool for diagnosis, categorization of lymphatic obstruction severity, and selection of appropriate treatment in extremity lymphedema patients.
This chapter focuses on the clinical application and interpretation of lymphoscintigraphy for the diagnosis and severity determination of extremity lymphedema, patient selection for appropriate treatments, and the evaluation of treatment outcome.
Diagnosis and Severity of Lymphedema: Clinical and Lymphoscintigraphy Findings
Diagnosis of Lymphedema
Patients with limb swelling are often commonly described with the term lymphedema regardless of the underlying cause. However, lymphedema, which may be primary or secondary, is a unique disease with specific clinical and imaging findings. Nonetheless, 25% of patients referred to a lymphedema service with the diagnosis of “lymphedema” have another disease.
The differential diagnosis of lymphedema is broad, which includes obesity, lipedema, infection, primary/recurrent malignancy, vascular anomalies, and systemic diseases such as congestive heart failure, hepatic failure, renal failure, hypoproteinemia, electrolyte imbalances, and peripheral neuropathies. The astute clinician should be able to accurately diagnose extremity swelling among multiple etiologies. Providing a correct diagnosis of the limb swelling is key before starting a treatment plan and establishing an objective baseline.
A thorough history and physical examination are the essential first steps to establishing a correct diagnosis of lymphedema. In most cases, the causes of primary and secondary lymphedema can be easily identified in the patient’s history. The clinical presentation is characterized by limb heaviness, swelling, tissue thickening, paresthesia, and recurrent cellulitis accompanied occasionally by localized pain. Initially, pitting edema is present in the distal limb and changes to non-pitting edema with the progression of the disease due to the collection of subcutaneous adipose and fibrosis. The Stemmer sign is commonly used for the clinical diagnosis of lymphedema. Noticeably, these clinical findings could result from a variety of diseases, and the diagnosis of lymphedema is not always correct.
Simultaneous assessment of the venous and lymphatic system is essential for a precise diagnosis. Duplex ultrasonography should be performed first in all forms of lymphedema to differentiate between lymphatic and venous etiologic factors or for the diagnosis of concomitant vascular anomalies. In the senior author’s routine practice, computed tomography (CT) angiography is used to diagnose vascular lesions if there is a suspicious clinical examination finding (e.g., cutaneous evidence of hemangioma, vascular malformation, or a palpable thrill).
Since 2018, in our lymphedema center, single photon emission computed tomography (SPECT) and magnetic resonance imaging (MRI) have been added for the diagnosis of chylous ascites secondary to retroperitoneal lymphangiomatosis.
Lymphedema Grading
The International Society of Lymphology (ISL) staging system is commonly used by the medical community. It is based on subjective and objective symptoms of edema. Briefly, stage 0 (latent lymphedema) represents lymph flow impairment after injury without swelling or visible signs of edema; stage 1 (spontaneously reversible lymphedema), assessable swelling or edema that resolves with elevation or conservative treatment; stage 2 (spontaneously irreversible lymphedema), progression of edema that does not adequately respond to compressive treatment; and stage 3 (lymphostatic elephantiasis), severe irreversible swelling, adipose deposition, and fibrosis resulting in thickened, firm skin, and hyperkeratosis. However, the ISL staging system does not reflect abnormal lymphatic circulation, and its application for surgical patients and outcome tracking is unreliable.
Circumferential or volumetric limb measurement is generally considered one of the objective clinical findings used to assess lymphedema status. Several modalities have been proposed to define the limb volume changes in lymphedematous limbs, including tape circumferential measurements, perometry, water displacement, and CT. In the senior author’s practice, circumferential measurements are taken based on anatomic locations: in the upper limb, 10 cm proximal and distal to the elbow; in the lower limb, 15 cm proximal and distal to the knee and 10 cm proximal to the ankle. These measurements are compared between the affected and the healthy limbs, allowing quantitative analysis of lymphedema and a method to follow the volume change with time. One of the criticisms of using tape measurements is that they are not as accurate as volumetric measurements. However, a recent study has shown a significant correlation between tape circumferential measurements and CT volumetric measurements.
Several other staging systems based on clinical symptoms, circumferential measurements, physiologic measurements, or a combination of clinical and imaging findings have been proposed. The Cheng Lymphedema Grading system is a five-grade system based on objective clinical and imaging findings to assess the severity of extremity lymphedema and to guide surgical treatment. The five grades are stratified essentially on the circumferential difference as follows: grade 0, <9%; grade I, 10–19%; grade II, 20–29%; grade III, 30–39%; and grade IV, >40%.
Lymphoscintigraphic Criteria for the Diagnosis of Lymphatic Dysfunction: Qualitative and Quantitative Analyses
Several imaging modalities can be used to aid in the diagnosis of lymphedema, such as lymphoscintigraphy, CT, MRI, and indocyanine green (ICG) lymphography. Both the ISL and the International Union of Phlebology recommended lymphoscintigraphy as the standard criterion for the diagnosis of lymphedema. This imaging modality is crucial not only to confirm whether lymphedema is present but also to document the severity of the lymphatic obstruction, which is critical for patient selection regarding treatment and for follow-up evaluation.
Radionuclide lymphoscintigraphy enables both qualitative and quantitative analyses to be performed. Visual qualitative information primarily aims to demonstrate the morphology of the lymphatic system by visualizing the lymph nodes and lymphatic ducts. Common qualitative findings for identifying lymphatic dysfunction include (1) symmetry, uptake intensity, number, and appearance timing of proximal lymph nodes (e.g., axillary or inguinal), (2) number and course of lymphatic ducts, (3) collateral lymphatic channels, (4) visualization of deep lymph nodes (e.g., elbow, popliteal), and (5) presence of dermal backflow.
Some authors have suggested 10–30 minutes as the standard time taken by the radiotracer to symmetrically reach the proximal axillary lymph nodes from the injection site. Delayed transport is considered at 60 minutes, and very compromised transport is considered at 120 minutes. However, a recent study showed that 120 minutes was the most frequent time necessary to visualize axillary lymph nodes in both melanoma patients before lymph node dissection and healthy volunteers.
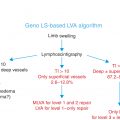
Vaqueiro et al. showed the usefulness of lymphoscintigraphy for the visualization of patent lymphatic ducts. Lymphoscintigraphy is able to visualize the number and course of lymphatic ducts. The detection of linear, engorged, or absent distal linear lymphatic ducts is a useful finding for planning lymphovenous anastomosis (LVA).
Dermal backflow findings are considered to be the abnormal extravasation of lymphatic fluid from the lymphatics into the interstitial space as a result of the incompetence of the deep lymphatic valves. Attempts have been made to grade the severity of dermal backflow. If untreated, dermal backflow with long symptom duration can extend from the distal limb to the entire limb as a sign of progressive limb lymphedema.
Visualization of lymph nodes in the elbow or knee is commonly considered an abnormal finding due to the routing of lymph flow from the superficial system to the deep system. However, other studies have described the presence of popliteal or epitrochlear nodes in “normal” subjects following the subcutaneous injection of radiotracer.
Hassanein et al. reported 96% sensitivity and 100% specificity for the diagnosis of lymphedema using qualitative information. In cases with a high suspicion of primary lymphedema and negative lymphoscintigraphies, the authors suggested repeating the test at least 1 year later.
Quantitative lymphoscintigraphy commonly focuses on (1) proximal lymph node uptake, (2) clearance of the radiopharmaceutical from the injection site or from anatomic limbs, and (3) appearance of the soluble molecules in the blood and various other calculations. Previous studies have used quantitative analyses to assess the severity of lymphatic obstruction following breast cancer treatment as well as to evaluate the treatment outcome in patients with lower limb lymphedema. The quantification is particularly useful when comparing the affected limb with the contralateral limb to verify if a preexisting lymphatic obstruction is already present due to a primary impairment. However, quantitative lymphoscintigraphy has often been criticized for inconsistent results and being time-consuming.
Lymphoscintigraphy Findings in Primary and Secondary Lymphedema
Different patterns of lymphoscintigraphy findings were found in primary and secondary lymphedema. Common patterns observed in primary lymphedema are high accumulation of radiotracer in the injection site, poor definition of the lymphatic vessels, delayed or absent visualization in the proximal lymph nodes, and, rarely, accumulation of radiotracer in soft tissue or lymphatic vessels in cases of hypoplasia or absence of radiotracer accumulation in case of aplasia. In secondary lymphedema, decreased or absent lymphatic transport and accumulation of radiotracer in soft tissue and lymphatic channels are the most common lymphoscintigraphic patterns. Some authors reported that lymphoscintigraphy cannot differentiate primary and secondary lymphedema.
Staging/Scoring Systems of Lymphoscintigraphy for the Diagnosis and Severity Determination of Lymphedema
In the medical literature, quite a few lymphoscintigraphy staging or scoring systems have been reported for the diagnosis and severity of extremity lymphedema ( Table 6.1 ). However, application of these tools in routine practice is variable due to their complexity and unclear correlation with lymphedema severity.
| LG Protocol | Clinical Criteria | Staging/Scoring | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Extremity | 99m Tc | Dose | Route | QI | Qn | Exercises | Images | LG Findings | Validation | Results | Treatment | Outcome | |||
| Kleinhans et al. | 81 |
| SSC | 75–110 MBq | s.c. | – | þ | þ | Dynamic up to 4 hours | – |
|
| 179 investigations
| 122 cases
| ALT (n=23) | TI: Mean↓ 5.9 |
| Cambria et al. | 188 |
| ASC | 503 µCi | s.c. | – | þ | þ | Dynamic | Subjective |
|
| – |
| – | – |
| Szuba et al. | 19 |
| SC | 0.25 mCi | s.c. | þ | þ | þ |
| – |
| 0–8 | – |
| CDT (n=19) |
|
| Lee and Bergan | 220 |
| ASC | N/A | N/A | þ | – | N/A | N/A | Subjective |
| Four stages | – | Broad overlapping between clinical and LG staging | CDT |
|
| Pecking et al. | 4328 |
| NC | N/A | s.c. | þ | – | þ | Dynamic:
| ISL (0–III) | Qualitative:
| Four stages (L0–L3) | – | Clinical and qualitative LG results not in accordance | – | – |
| Gebouský et al. | 88 |
| SC | 20 MBq | s.c. | þ | þ | þ |
| Subjective scale, 0–4 | Qualitative:
| Five stages (0–4) | – | LG and the clinical staging coincided in 78.9% of cases | – | – |
| Maegawa et al. | 142 |
| HSA | 40 MBq | s.c. | þ | – | – |
| ISL (0–III) |
|
| – |
| LVA (n=35 limbs/31 patients) |
|
| Mikami et al. | 78 |
| HSA | 40 MBq | s.c. | þ | – | – |
| ISL (0-III) |
| Five types, three subtypes | – |
| LVA (n=20) |
|
| Dylke et al. | 57 |
| ASC | 20–30 MBq | i.d. | þ | – | – | Static:
| – | Dermal backflow:
| Szuba 4-point Dermal Backflow Scale | Intraobserver reliability: k =0.418, SE=0.008 |
| – | – |
| Ebrahim et al. | 81 |
| NC | 20 MBq | s.c. | þ | – | – | Static
| – | Eight criteria:
|
|
| – | – | – |
| Cheng et al. | 285 |
| PT | 37 MBq | s.c. | þ | – | þ | Static
|
|
|
|
| TLS
|
| Surgical group
|
Related posts:
 Anatomy and Structural Physiology of the Lymphatic System
Anatomy and Structural Physiology of the Lymphatic System
 Refining Planning of Lymphedema Surgery of the Extremities Using MRI and CT Imaging Techniques
Refining Planning of Lymphedema Surgery of the Extremities Using MRI and CT Imaging Techniques
 Microsurgical Procedures: Vascularized Lymph Node Transfer from the Submental Region
Microsurgical Procedures: Vascularized Lymph Node Transfer from the Submental Region
 Private: The Campisi Approach for Lymphatic Surgery
Private: The Campisi Approach for Lymphatic Surgery
 Private: Tracking Outcomes Following Lymphedema Treatments
Private: Tracking Outcomes Following Lymphedema Treatments
 Private: Microsurgical Procedures: Vascularized Lymph Node Transfer from the Thoracodorsal Axis
Private: Microsurgical Procedures: Vascularized Lymph Node Transfer from the Thoracodorsal Axis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


