| Lower eyelid retraction with volume loss |
| Posterior lamellar and/or middle lamellar shortening |
| Desire for use of autologous grafts |
| HIV-associated lipoatrophy |
| Prostaglandin-associated lipoatrophy |
| Lower eyelid retraction seen in craniofacial syndromes (ie Treacher Collins syndrome) |
| Assess for volume loss/hollowing of lower eyelid |
| Quantify amount of eyelid retraction according to MRD2 |
| Manual palpation and elevation of lower eyelid to feel for restriction; if supple elevation is possible, spacer may not be required |
| Assess adequacy of anterior lamella; may need cheek lift or skin graft if severe shortening |
| Assess eyelid laxity |
| Assess inferior orbital rim and presence of negative vector |
| Assess orbicularis strength; weakness on closure may portend high risk of recurrence |
| Prior eyelid, facial surgery or trauma |
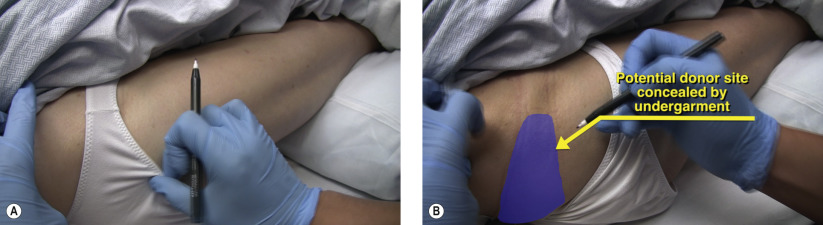
| Suitability for donor site of dermis fat (retro/preauricular, hip/gluteal, flank/periumbilical) |
Introduction
The use of dermis fat as a posterior lamellar graft for lower eyelid reconstruction has several advantages over acellular dermis and hard palate. Dermis fat can provide a virtually limitless amount of volume augmentation and surface area compared to acellular dermis ( Chapter 34 ) and hard palate ( Chapter 36 ). Dermis fat is autologous, which may appeal to patients who are adverse to use of xenografts. Hard palate, although autologous, has more associated donor site morbidity, such as postoperative pain, difficulty eating, and potential for fistula formation compared to dermis fat. The use of dermis fat, acellular dermis, and hard palate is technically similar and review of each of these chapters ( Chapter 34 , Chapter 36 ) should be performed to appreciate the subtle nuances of each graft.
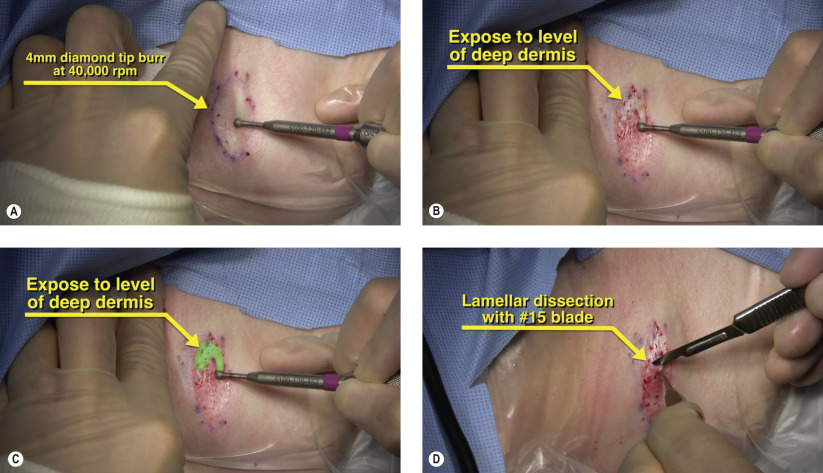
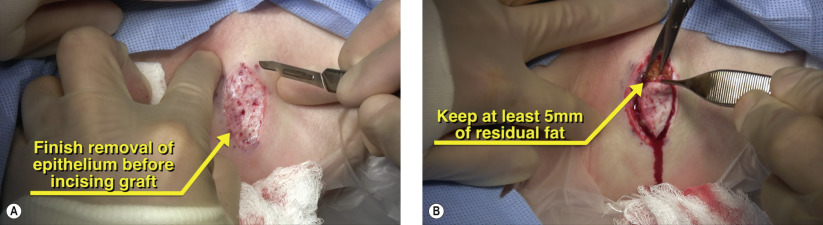
Surgical Technique
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


