| Upper or lower eyelid defect from skin cancer removal |
| Scarring or notching of eyelid |
| Focal entropion or madarosis causing functional or aesthetic concerns |
| Size and dimensions of defect |
| Age of patient |
| Eyelid laxity |
| Prior eyelid, facial surgery or trauma |
Introduction
Reconstruction of eyelid defects requires the surgeon to have an artistic intuition with regard to balancing structure, function and aesthetics. Many factors will shape the final decision as to the type and technique of reconstruction. This is influenced by the age of the patient, degree of skin and eyelid laxity, visual factors (monocular versus binocular status), and surgeon preference.
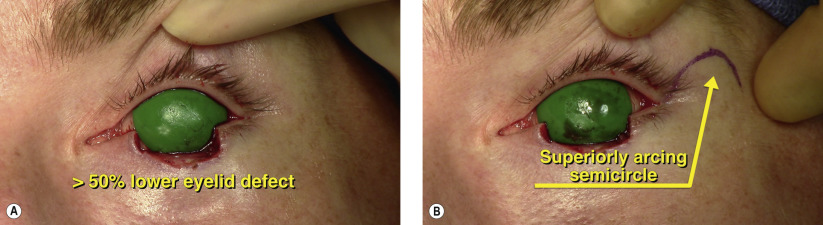
The goals of any eyelid reconstruction should be to recreate the bi-lamellar structure with a smooth eyelid margin and contour, preservation of the normal vertical excursion and appropriate horizontal tension. Depending on the amount of horizontal laxity, a semicircular flap can be useful in defects ranging in size from 30 to 60% of the horizontal eyelid length. With greater amounts of laxity, even larger defects can be reconstructed.
Originally described by Tenzel in 1975, the semicircular flap remains a workhorse in the surgical repertoire for both upper and lower eyelid reconstruction. The advantages of the procedure include the re-creation of the normal bi-lamellar eyelid architecture without the use of grafts, an unoccluded visual axis for use in monocular patients and optimum cosmesis. The disadvantages include the potential for scarring in the soft tissues lateral to the canthus, a non-cilia-bearing reconstructed eyelid segment laterally, and the potential for notching at the reconstructed juncture of the native and advanced eyelid segments.
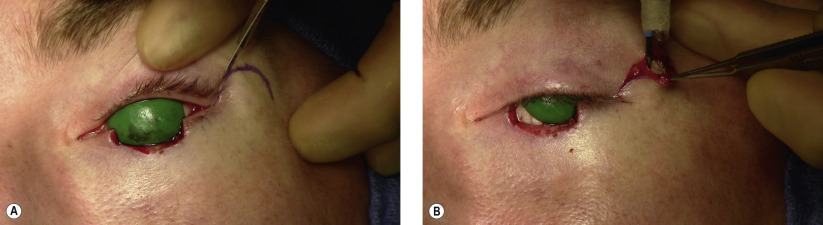
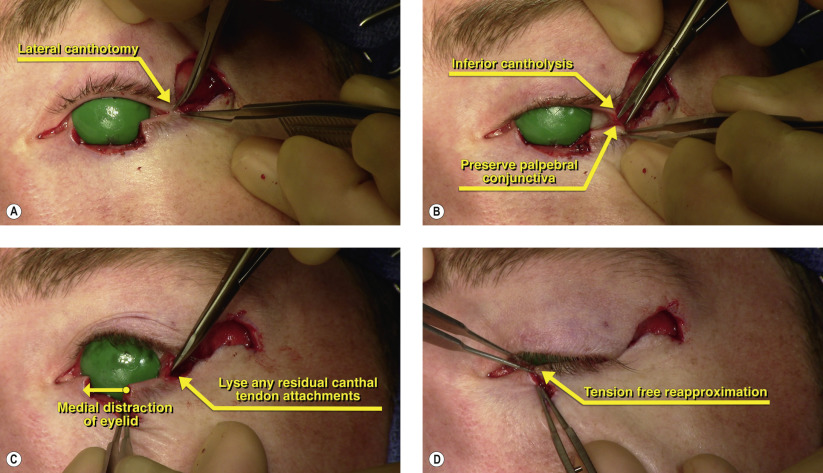
Surgical Technique