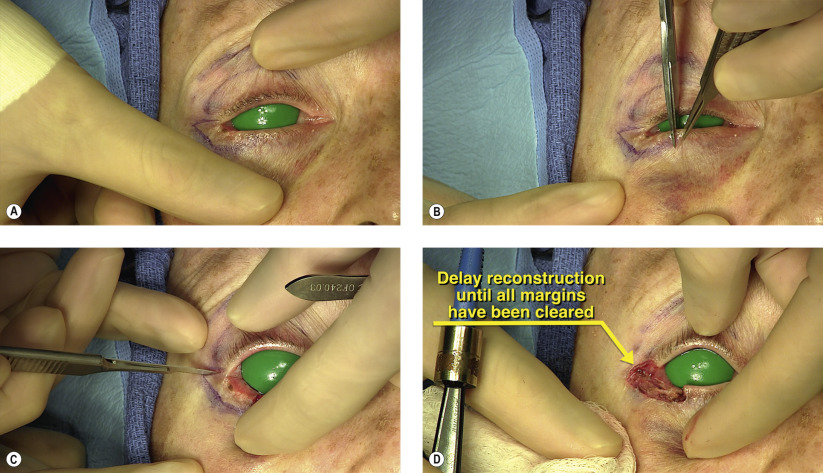
| Lower eyelid defect from skin cancer removal (30–50% defect) |
| Scarring or notching of eyelid |
| Focal entropion or madarosis causing functional or aesthetic concerns |
| Size and dimensions of defect |
| Age of patient |
| Eyelid laxity and availability of upper eyelid redundancy |
| History of eyelid, facial surgery or trauma (prior upper blepharoplasty may limit availability of adjacent tissue flap) |
Introduction
The size and location of eyelid defects typically dictate the reconstructive options available to the surgeon. Defects that are less than 25% typically can be closed primarily. The bi-lamellar anatomical structure of the eyelids allows the surgeon a multitude of choices to restore structure, function, and optimal appearance.
Anatomically, the redundant vascular supply permits random anterior lamellar flaps. A dual vascular arcade supplies the eyelid, one located at the eyelid margin and the other peripherally along the tarsal border. This has adjacent collateral contributions from the supply of the medial palpebral artery from the angular and the zygomatico-orbital branch of the superficial temporal artery. The rich vascular flow to the periocular region enables creative flap construction that is unparalleled in other areas of the body.
A central continuous lash-bearing segment typically gives the best aesthetic result. It is less conspicuous if the non-lash-bearing segment is located laterally and not centrally. For this reason, with lower eyelid defects greater than 50% of the eyelid margin not involving the canthus, the semicircular flap is typically our preferred approach ( Chapter 39 ).
In cases of larger defects with lateral canthal involvement, several possibilities exist. Some of the options are: tarsoconjunctival pedicle from the upper eyelid with anterior lamellar flap ( Chapter 40 ); full thickness skin graft ( Chapter 27 ); Mustardé cheek rotational flap ( Chapter 41 ); and free posterior lamellar graft with periocular adjacent anterior lamellar flap ( Chapter 43 ). If the surgeon is using an upper eyelid pedicle flap, orbicularis can also be transferred for additional volume.
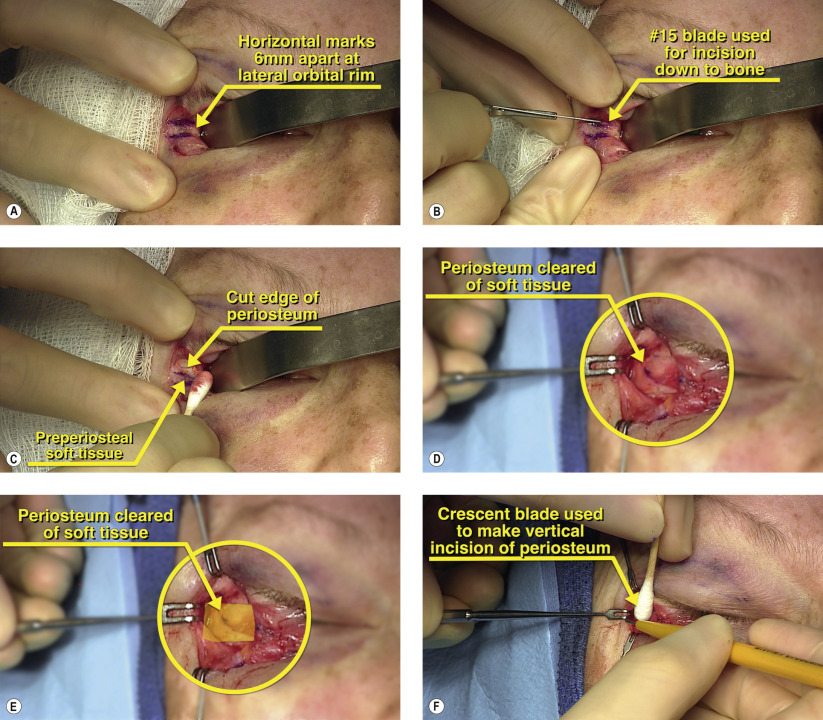
The periosteum along the lateral orbital rim is unique in that it provides an anchor point for the medial eyelid remnant and can serve as the posterior lamella. It can be harvested and shaped to fit a particular-sized defect and provides adequate vascularity to support a free skin graft if necessary. If an anterior lamellar flap is used, an additional vascular supply is provided. The periosteal flap can also be used to reconstruct the inferior fornix as the palpebral conjunctiva can be advanced superiorly and secured to the inferior portion of the periosteal flap.
The advantages of the procedure include: the recreation of the normal bi-lamellar lid structure, an unoccluded visual axis for use in monocular patients, and an excellent aesthetic appearance. The disadvantages include: a non-cilia-bearing reconstructed eyelid segment laterally, and the potential for notching or scarring at the reconstructed juncture of the native and advanced eyelid segments.
Surgical Technique