Introduction
The lips constitute the main feature of the lower third of the face, and have been a focus of interest by reconstructive, cleft, and esthetic surgeons. Functionally, the lips play many important roles – articulation and enunciation in speech; maintenance of oral competence during eating, drinking, and forceful blowing; and expression of emotion and kissing. These roles are possible because, unlike the other elements of the face, the lips are dynamic and mobile. Esthetically, the vermilion is the hallmark; discrepancies of 1 mm are noted by the naked eye across the room. Reconstruction of the lips, therefore, aims to maintain these characteristics both for function and appearance.
This chapter reviews the anatomy of the lips and presents an algorithm for reconstruction.
Anatomy
Embryology
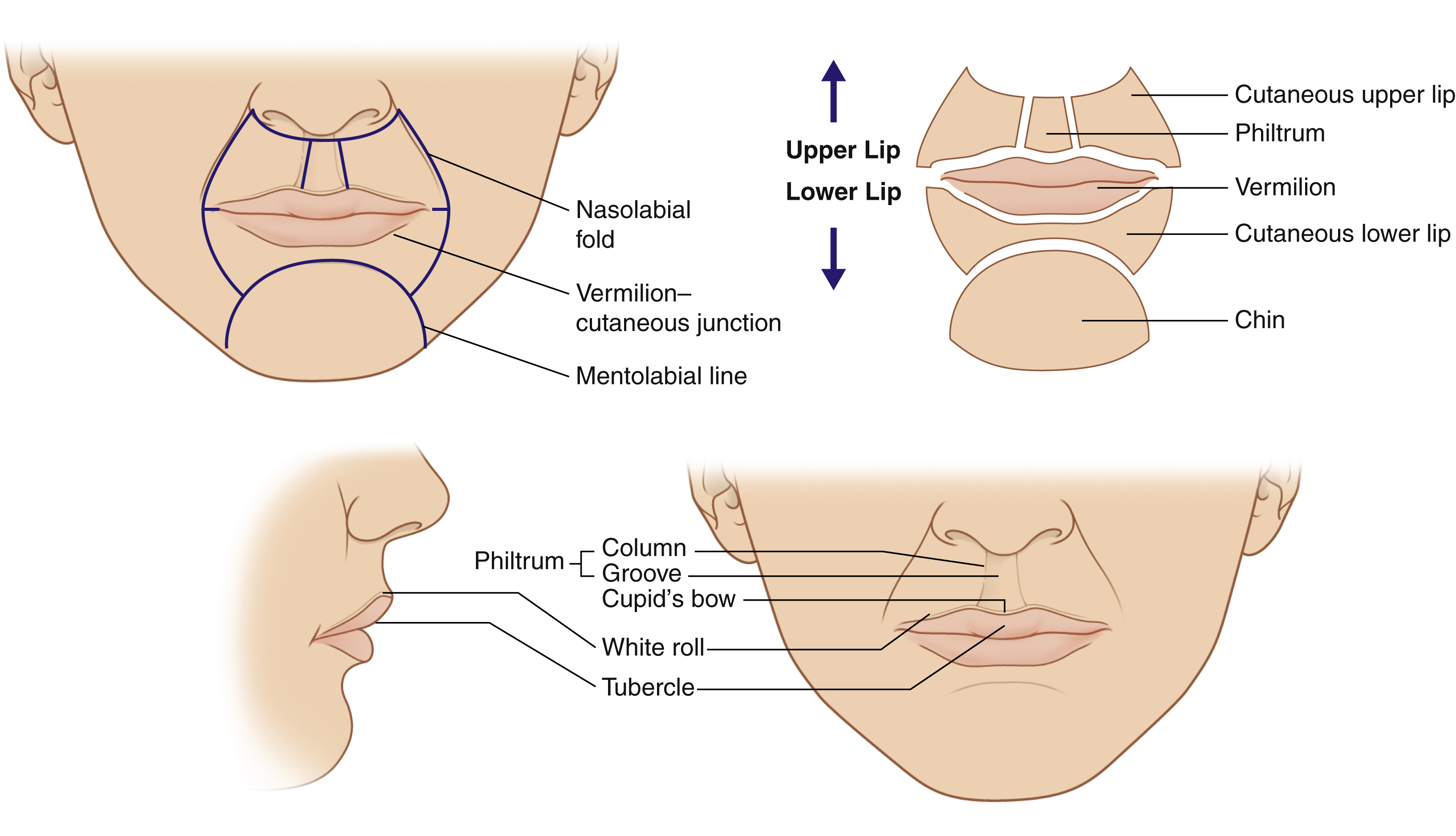
The upper lip is derived from two distinct structures, namely the paired maxillary and nasomedial processes. Fusion of these processes gives rise to the characteristic features of the upper lip, such as the philtral columns, philtral dimple, Cupid’s bow and white roll. The lower lip is formed from fusion of the paired mandibular processes, which result in a less defined lower lip. The topographical landmarks of the lip are illustrated in Fig. 29.1 .
Musculature
The muscles that animate the lips are illustrated in Fig. 29.2 . The principle muscle is the orbicularis oris, which forms a complex sphincter muscle. This muscle arises both from intrinsic fibers of the lip as well as from other muscles which insert into the lip. The deep and oblique fibers of orbicularis oris approximate the lips to the alveolar arch, while the superficial fibers purse and protrude the lips. The orbicularis oris can be dissected from its supportive muscles while preserving its viability, sensation, and motor function, an important consideration in the choice of reconstruction.
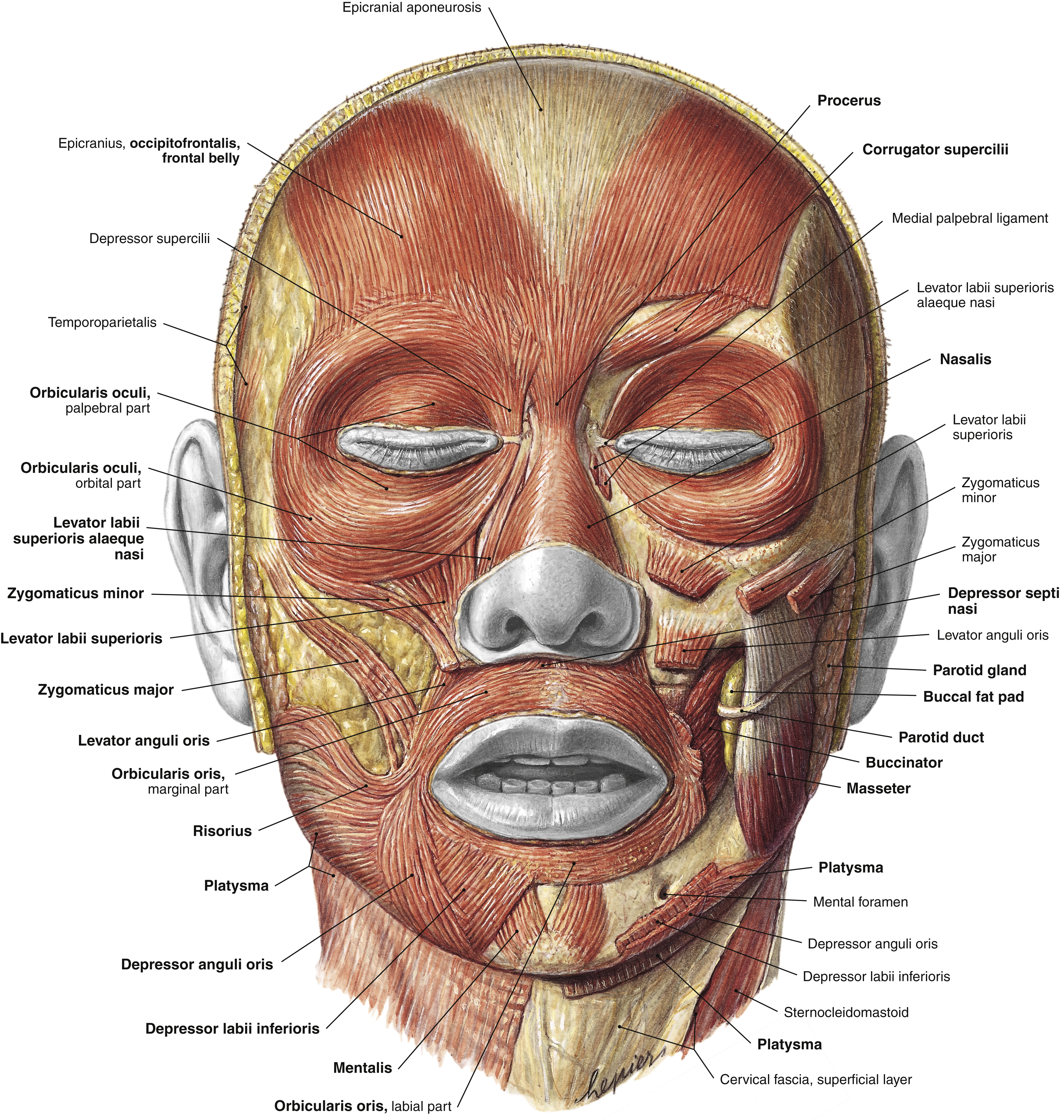
Levator labii superioris elevate the upper lip, levator anguli oris and zygomaticus major draw the lateral upper lip up and back, while buccinator and risorius clear the gingival sulcus. The lower lip is depressed and retracted by the platysma, depressor anguli oris, and depressor labii inferioris. The mentalis muscles cause elevation and protrusion of the central aspect of the lower lip. Loss of these muscles leads to lip incompetence and incisor show.
Vasculature
The blood supply to the upper and lower lips is the superior and inferior labial arteries, respectively. These originate from the facial artery from either side of the face. The average distance of the superior labial artery from the oral commissure (as it branches off the facial artery) is 12 mm, and can be found along its course within 10 mm from the inferior border of the lips. However, the anatomy of the labial arteries can be variable. Magden et al reported that 29% of superior labial arteries have a unilateral origin. This finding has important implications when raising pedicled flaps, such as the Abbe or Estlander flaps. The superior labial artery has a mean diameter of between 1 and 2 mm at its origin, and is therefore large enough for microsurgical anastomosis. , There are numerous reports and case series of lip replantation in the literature, and problems attributed to replantation are mainly related to the venous drainage of the replanted tissue.
The origin of the inferior labial artery varies between the lower margin of the mandible and the oral commissure.
Lymphatic Drainage
The lymphatic drainage of the lips is ipsilaterally into the submental, submandibular, and parotid nodes. Tissues in the midline drain bilaterally. Submental lymph nodes then drain into ipsilateral submandibular nodes. Submandibular and parotid nodes secondarily drain into the ipsilateral jugulodigastric lymph nodes.
Innervation
The facial nerve (VIIth cranial nerve) provides the motor innervation to the perioral musculature via its buccal and marginal mandibular branches. There are interconnections between both branches of the facial nerve distal to the parotid gland. The motor nerves are located on the undersurface of all the perioral musculature except for buccinator, levator anguli oris, and mentalis, where the nerve lies on the superficial surface of these muscles.
The maxillary and mandibular branches of the trigeminal nerve (Vth cranial nerve) provide sensory innervation to the perioral region. Specifically, the infraorbital nerve, which is a terminal branch of the maxillary nerve, innervates the upper lip. The infraorbital foramen faces downward and medial and lies 4–7 mm below the infraorbital rim, on a vertical line that descends from the medial limbus of the iris. The nerve runs beneath the levator labii superioris and superficial to the levator anguli oris to supply the lateral nasal sidewall, ala, columella, medial cheek, and upper lip. The lower lip, down to the labiomental fold, is innervated by the mental nerve, which originates from the inferior alveolar nerve, a branch of the mandibular nerve. The mental foramen is located below the apex of the second mandibular bicuspid with 6–10 mm of lateral variability.
Etiology of Lip Defects
The commonest indication for lip reconstruction is following tumor extirpation. The lower lip is much more frequently affected by neoplasia compared to the upper lip, presumably due to greater actinic exposure. The vast majority of skin cancers are squamous cell carcinoma in origin and are more frequently encountered in males (2.4 times) as a result of greater sun exposure, alcohol, and tobacco. Fortunately, these lesions often involve the area between the midline and the oral commissure, avoiding the need for commissural reconstruction. Other causes of lip defects include trauma, infection (e.g., noma), vasculitis, and congenital causes such as vascular malformation or clefts.
Reconstruction: General Principles
Goals
The three main goals of lip reconstruction are:
- 1.
Preservation of oral continence – this requires a muscular integrity, normal sensation and an adequate oral aperture.
- 2.
Preservation of function for speech and ingestion of food.
- 3.
Cosmesis.
Anesthesia
Surgical procedures to the perioral region should be preceded by a regional block, followed by local infiltration to the affected area for the adrenaline-facilitated vasoconstriction. Prior to local infiltration of the lip tissue, it is important to mark or tattoo the white roll of the lip either side of the planned resection in order to match this up afterwards. Any local infiltration, particularly with adrenaline, will obliterate the white roll. A 1-mm discrepancy between the vermilion and skin is noticeable at conversational distance.
The entire upper lip can be anesthetized by bilateral infraorbital nerve block. This can be carried out either percutaneously or transorally. A 25–27G needle is used and does not need to pass into the foramen to desensitize the lip. For the percutaneous route, the needle is placed medial to the nasolabial fold but lateral to the alar base. For the transoral route, the needle is passed transmucosally above the canine eminence.
The lower lip is anesthetized by bilateral mental nerve blockade. This is performed intraorally by rolling the lower lip outward and stretching the mucosa to visualize the mental nerve just below the mucosa at the canine root. If the nerve is not readily visible, the surgeon should infiltrate local anesthetic into the submucosa at the apices of the canines into the lower lateral buccal sulcus.
Analysis of the Defect
Before embarking on lip reconstruction, the following factors need to be contemplated.
Site
The upper lip has more topographical landmarks compared to the lower lip. The lower lip, lacking in features, is theoretically more expendable as donor tissue for reconstruction. However, functionally and socially, the lower lip deserves more consideration. The lower lip serves to maintain oral competence by containing solids and liquids within the oral cavity. Therefore, any reduction in sulcus depth, compounded by loss of sensation and poor muscle function, will result in liquids leaking out of the mouth. The lower lip can be thought of as one subunit and the upper lip can be thought of either as two subunits (left and right) or as three (two laterals and a central).
Hence, the surgeon needs to deliberate carefully in the following situations: using lower lip tissue to reconstruct the upper lip, denervating the lower lip during the raising of local flaps, or the use of insensate and nonfunctional tissue such as the nasolabial or cheek tissue to reconstruct the lower lip.
Size
Whilst the absolute size of the tumor and excision margins is important, the percentage of the lip which has been ablated is crucial in deciding the reconstructive option. As previously mentioned the lower lip is more expendable, especially in elderly patients with more laxity in the tissues, thereby permitting transposition, advancement or rotation flaps more readily. However, it is vital not to leave the patient with a microstomia. Although amenable to stretching, microstomia does result in imminent problems with dental care, insertion and removal of dentures.
Depth
The four layers of the lip from the oral cavity outwards are mucosa, muscle, vermilion, and skin. With regards to the depth of the defect, the surgeon should “replace like with like” and consider the reconstructive options accordingly.
Involvement of Commissure
If the lip defect involves the oral commissure, then effort must be made to reconstruct the commissure as this is an important esthetic landmark of the lips and face.
Algorithm for Reconstruction
Vermilion Defects
The vermilion is a unique feature of the lip. The vermilion is the transition zone between the stratified keratinized squamous epithelium of the skin and the nonkeratinized squamous epithelium of the oral mucosa. This exists only in humans, and is the partially keratinized layer, which is red due to the reflection of the underlying blood vessels. The wet and dry vermilions are distinct, and in women, the dry vermilion tends to take on lipstick more readily.
For small lesions confined within the vermilion, the lesion should be excised as a vertical ellipse and sutured directly avoiding extension of the incision onto the skin. This technique can also be employed for notch or whistle deformities of the lip, with the addition of a Z -plasty to avoid recurrence.
Large superficial defects confined to the vermilion can be left to heal by secondary intention, and tend to heal within 3–4 weeks with a good cosmetic result.
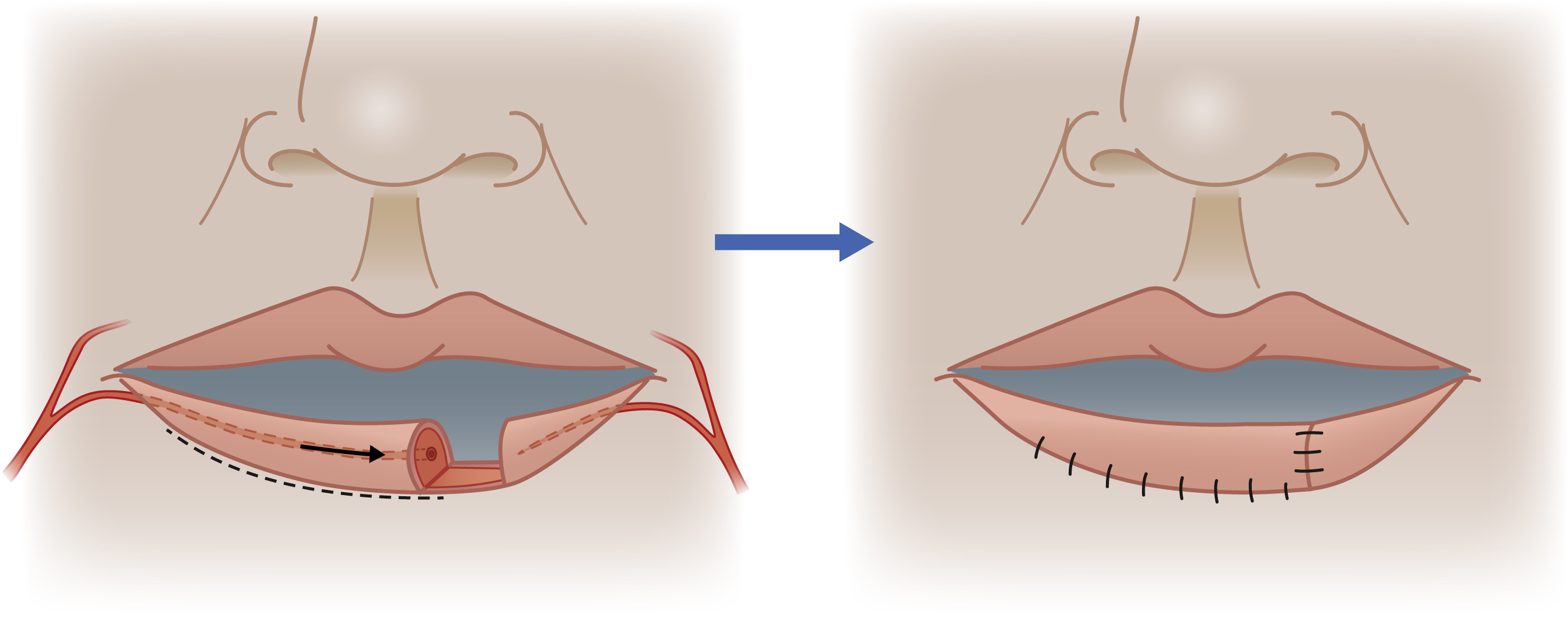
For full-thickness defects resulting in a deficiency of less than 50% of the total vermilion, the options include the axial musculovermilion advancement flap described by Goldstein or a musculomucosal V–Y advancement flaps. For the axial musculovermilion advancement flap, the position of the labial artery is identified from the resection of the lesion and the flap is elevated deep to the labial artery, and then advanced into the defect ( Fig. 29.3 ). Although cross-lip flaps for vermilion reconstruction have been widely reported in the literature, it is our opinion that they should be avoided. Cross-lip flaps should not be undertaken lightly as they not only compromise the other intact lip, but also are difficult to tolerate as they are executed as a staged procedure with an intervening period of lip adhesion, i.e., the pedicle of the flap attached.
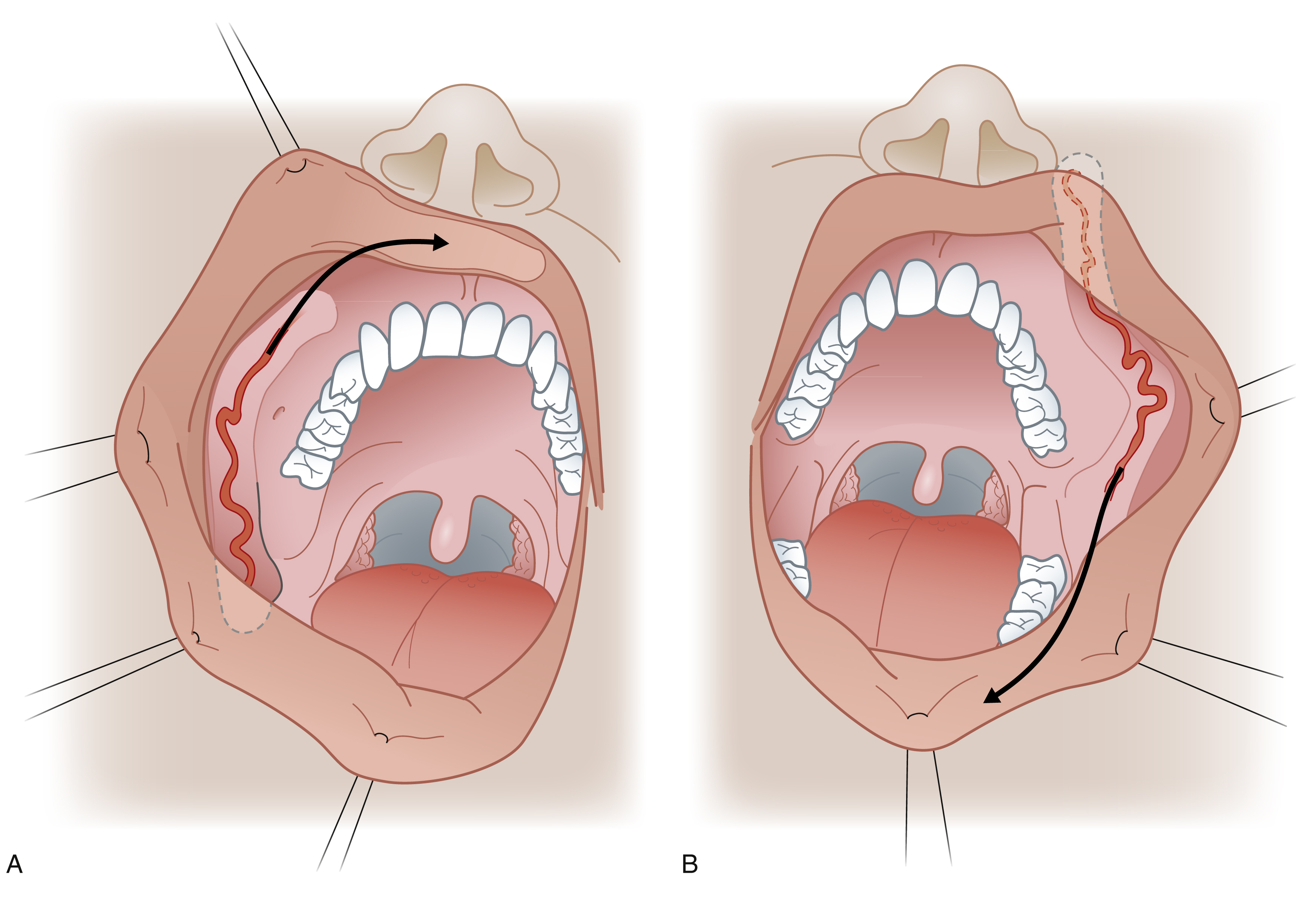
The facial artery myomucosal flap (FAMM) described by Pribaz in 1992 is a good option for vermilion defects of more than 50%.This flap can also be used for total vermilion reconstruction by raising bilateral flaps. The FAMM flap is a composite flap, which is raised from the lateral cheek, based on the facial artery as it courses though the cheek lateral to the buccinator muscle. It consists of mucosa, submucosa, a small amount of buccinator, a segment of the facial artery and venous plexus. It may be used as a superiorly based flap, which has retrograde perfusion via the angular artery, for the upper lip. Alternatively, the inferiorly based flap based on the facial artery is used for the lower lip. Wide flaps, up to the entire width of the cheek, and up to 7–8 cm in length, can be raised safely but the authors advocate thin flaps to reduce donor site morbidity ( Fig. 29.4 ).