Lip Adhesion
Catharine B. Garland
Jesse Goldstein
Joseph E. Losee
DEFINITION
For infants with complete unilateral or bilateral cleft lip, lip adhesion is an alternative to presurgical infant orthopedics (PSIO).
Any child with a wide complete cleft lip may be a good candidate for some form of presurgical intervention to reduce tension and optimize symmetry prior to repair.
Presurgical interventions include the following:
Lip adhesion surgery, which converts a complete cleft lip into an incomplete cleft lip
ANATOMY
A complete cleft lip distorts both the lip and nose anatomy.
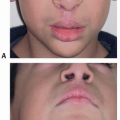
In the unilateral complete cleft lip (FIG 1):
The orbicularis oris muscle is not in continuity. In the lateral lip element, the orbicularis oris muscle inserts vertically into the alar base and piriform.
The alar base on the cleft side is typically positioned laterally, inferiorly, and posteriorly on the collapsed minor alveolar arch.
The caudal septum and columella are deviated to the noncleft side. The medial component of the orbicularis oris muscle inserts on these structures.

FIG 1 • Unilateral complete cleft lip and nose. Note inferior, lateral, and posterior positioning of cleft side alar base and deviation of columella. (Reprinted from Kirschner RE, Adetayo OA, Losee JE. Lip adhesion. In: Comprehensive Cleft Care. 2nd ed. Vol 2, Chapter 41. Boca Raton, FL: CRC Press; 2016:781-791, www.thieme.com, with permission.)
In the bilateral complete cleft lip (FIG 2):
The premaxilla is often displaced anteriorly and may be twisted or locked out of the transversely collapsed lateral maxillary segments.
The lateral maxillary segments are relatively retropositioned and often collapsed.
The orbicularis oris muscle is widely separated, inserting into the alar bases at the piriform bilaterally.
The alar bases are laterally displaced and often asymmetric.
The columella is shortened.
Normalizing some of this anatomy prior to definitive lip repair may improve the outcomes of surgery with regards to lip and nose symmetry.
PATIENT HISTORY AND PHYSICAL FINDINGS
The sequence of surgical intervention for a complete cleft lip depends on individual patient and family characteristics and the surgeon and cleft center experience. This determines whether a patient undergoes a single-stage lip repair, lip adhesion prior to formal lip repair, or PSIO prior to lip repair.
On physical examination, the width of the cleft, the presence of nostril sill tissue (a Simonart band), the relationship of the major and minor alveolar segments in the unilateral cleft lip, or the size and position of the premaxilla in the bilateral cleft lip are all evaluated carefully.
Patient history must include an assessment of the infant’s feeding and growth and identification of any medical comorbidities that may alter treatment.
Family characteristics that factor into decision-making include financial, geographic, or other constraints. These may influence the parents’ ability to frequently travel for PSIO or to be compliant with the daily care required.
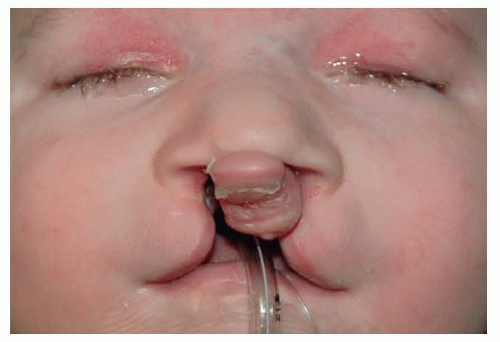
FIG 2 • Bilateral complete cleft lip and nose. Note wide alar bases, short columella, and the anterior displacement of the premaxilla relative to the lateral maxillary arches.
Determining whether an infant is a good candidate for a lip adhesion includes weighing the advantages and disadvantages with the family:
Lip adhesion will convert the complete cleft lip to an incomplete cleft lip and reduce the alveolar gap as well as tension on the final repair.5
Compared with nonoperative PSIO, which requires frequent office visits, lip adhesion can reduce the burden of care on the family.6
In the bilateral complete cleft lip, labial adhesion may retract the prominent premaxilla and help to lengthen the columella.7
Lip adhesion incurs the additional costs of a second operation6 and risks of an additional general anesthetic for the infant.
IMAGING
None needed
NONOPERATIVE MANAGEMENT
PSIO
Nasoalveolar molding (NAM)1: NAM is a passive technique that aligns the maxillary arches, narrows the alveolar gap, and molds the nasal cartilage. It is typically initiated within the first several weeks after birth. The infant must wear the device daily, and the orthodontist adjusts it weekly.
Latham device2,5: For the protruding premaxilla, the Latham device employs active lateral movement of the maxillary alveolar segments and retraction of the premaxilla posteriorly to realign the arch form.7 This is a more rapid repositioning than nasoalveolar molding but does require a general anesthetic for placement of the Latham device.
Single-stage cleft lip repair: Some authors argue that lip adhesion is an unnecessary procedure, despite the width of the cleft, and that equivalent results can be obtained in a single-stage repair.
SURGICAL MANAGEMENT
Indications for lip adhesion include patients with wide complete clefts who are unable to undergo nonsurgical PSIO.
Risks of surgery include infection, dehiscence, and scarring.
In the bilateral cleft lip and palate patient with a protuberant premaxilla, lip adhesion may be combined with a premaxillary setback to optimize alignment of the premaxilla. This is typically reserved for older patients whose tissues (ie, premaxilla) are unlikely to mold under the compression of the lip adhesion alone.
Preoperative Planning
All infants with a cleft must undergo full physical examination to rule out any concomitant cardiopulmonary disease or airway abnormalities. If additional medical problems are identified, genetic evaluation may be warranted.
After birth, feeding evaluation is performed by instructing parents in the use of specialized bottles as needed. Weight gain is monitored weekly to ensure that nutrition is adequate.
A complete blood count can be performed before surgery to evaluate for anemia of infancy. After birth, hemoglobin typically reaches a nadir between 8 and 12 weeks of life in healthy term infants. In premature infants, the nadir is more profound and occurs earlier.
Positioning
General anesthesia is induced, and the patient is intubated with an oral Rae tube, which is taped in the midline of the chin to prevent any distortion of the upper lip.
The patient is positioned supine with the head on a small gel donut.
Lubrication ointment is placed in the eyes.
The face is prepared with Betadine, and sterile drapes are applied.
Approach
Loupe magnification is used to optimize precision of the procedure.
The markings for a formal cleft lip repair are performed, as they would be at the time of definitive repair. Key points are tattooed with methylene blue.
Importantly, the alar bases and alar-facial grooves are marked, so that the adhesion will lead to both vertical and horizontal symmetry of these features.
The markings for the lip adhesion are then made within the tissues that would be discarded at the time of the formal repair or within the “L” and “M” flaps.
Some surgeons perform primary nasal repair at the time of lip adhesion, while others defer this until the time of the formal lip repair.
TECHNIQUES
▪ Unilateral Cleft Lip Adhesion
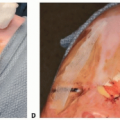
Markings
The unilateral cleft lip repair is marked and key points are tattooed. The alar bases and alar-facial grooves are marked (TECH FIG 1A).
Incisions for the labial adhesion are marked within the area of the vermillion that is normally discarded on both the medial and lateral lip element. The incisions are around 10 to 15 mm in length and symmetric (TECH FIG 1B,C). The inferior half of the incision is performed on the upper lip, and, the superior half is performed on the nasal floor—truly making this a “lip-nose adhesion.” On the medial lip element, the midpoint of the incision is centered at the columellar-lip junction. On the lateral lip element, the alar base denotes the midpoint of the incision. The position of these incisions is critical for alignment of the alar base. The alar base must be symmetric with the contralateral side in both the horizontal and vertical plane, or an asymmetric adhesion and repair will be performed and will make the subsequent definitive cleft lip and nose repair more challenging.
The lateral buccal sulcus incision is marked to mobilize medially of the lateral lip element and ultimately a tension-free adhesion. This incision is carried up around the piriform aperture to just above the inferior turbinate (TECH FIG 1D).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree