CHAPTER 31 Lid–cheek blending: the tear trough deformity
History
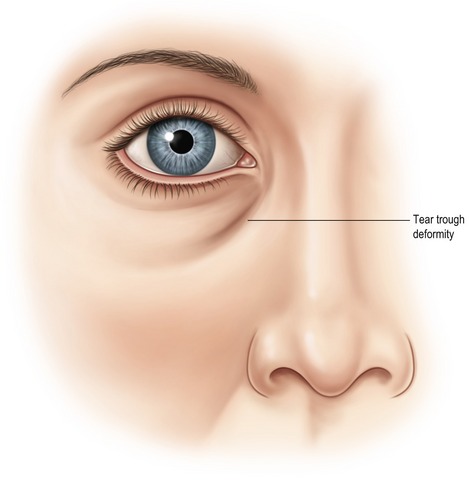
While traditional lower lid blepharoplasty has been performed in order to improve the periorbital region, the tear trough deformity should be considered a separate anatomical subunit of the lower periorbital aesthetic unit. One of the unique aspects of the tear trough deformity is that while it may be age related, the dark appearing groove associated with the deformity is often present in young patients with no other signs of periorbital aging (Fig. 31.1). The “tear trough deformity” was reportedly first named by Flowers in 1969 when he “[noticed] how a shed tear often tracks the course of this groove…” Flowers also credited Loeb who earlier, in 1961, adopted the descriptive term “nasojugal groove” from the ophthalmology literature by Duke-Elder. During the decade that followed, the terms became synonymous and both Loeb and Flowers published elegant surgical techniques aimed at correction of the deformity. Since it became apparent that fat removal was not successful at correcting the tear trough deformity, techniques evolved which were specifically aimed at correction of the tear trough deformity. Early techniques by Loeb in 1981 included fat pad sliding and fat grafting, while Flowers used orbicularis muscle plication, fat translocation, and subgaleal grafts. Disappointment with resorption of autogenous grafts led Flowers to develop alloplastic tear trough implants by 1993.
Physical evaluation
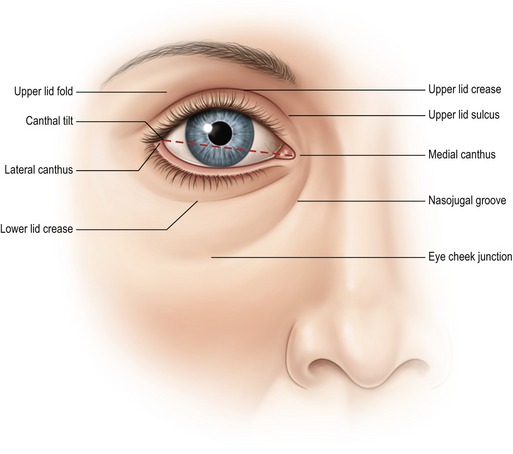
• Eyelid shape: relationship of the lower lid to the inferior corneoscleral limbus and the lid tilt based on the relationship of the lateral canthus and medial canthus (Fig. 31.2).
• Orbital morphology: vector analysis to determine morphologically prone eye, positive and negative vector, and Hertel exophthalmometry to determine globe prominence.
• Lower lid tone: lid snap back and lid distraction to evaluate orbicularis tone and tarsoligamentous laxity.
• Volumetric analysis: evaluation of excess skin, muscle and orbital fat with emphasis on the lid–cheek junction defined by the orbitomalar ligament and tear trough deformity, retropulsion of orbital fat.
• Midfacial aging: the presence of descent of the SOOF (suborbicularis oculi fat), malar fat pad, or the presence of malar bags or festoons.
• Skin analysis: evaluation of photoaging of the periorbital region including loss of elasticity, rhytids, and hyperpigmentation.
• Tear analysis: history of dry eyes, contact lens intolerance, and performance of Schirmer’s test for tear production.
Anatomy
Flowers described the tear trough deformity as the triangular shaped defect between the angular head of the quadratus labii superioris muscle and the orbicularis muscle. There is often associated deficiency of the infraorbital rim which Rees described as bony deficit below the normal rim or suborbital hypoplasia. The presence of excess orbital fat often disguises the tear trough deformity and distracts the surgeon’s attention. Since removal of excess orbital fat does not correct the tear trough, simulation of fat removal with retropulsion of the fat superiomedial to the tear trough clearly defines the anatomy of the defect. The defect can be considered a depression bordered by orbital portion of the orbicularis oculi, the levator labii superioris, levator alaeque nasi muscles (Fig. 31.3). Since there is little subcutaneous tissue between the skin and the orbicularis muscle, the tear trough is comprised of thin skin at the junction of eyelid, nasal and cheek skin with attenuated subcutaneous tissue overlying the maxilla. The tear trough can therefore be considered a defect of the anterior lamella with underlying bony contributions. The formation of the tear trough deformity is often one of the first signs of aging around the eyes. The concavity in the nasojugal groove is often associated with apparent fat herniation above or it may present independently. There is individual variation in depth and morphology of the tear trough and periorbital hollows along the rim. In order to devise the optimal correction for the tear trough, understanding the anatomy of this area is critical.
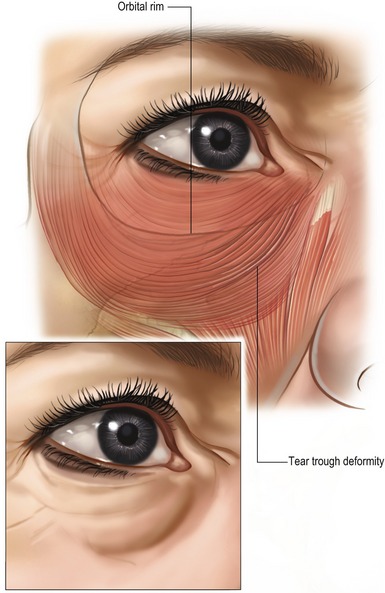
The orbicularis oculi muscle has a direct attachment to the inferior orbital rim from the anterior lacrimal crest to the medial limbus or approximately 30% of the length of the rim. Lateral to this, the attachment to the bone is via the orbicularis retaining ligaments (ORL) which have variable length at different points along the inferior orbital rim. The length increases to a maximum centrally and then decreases laterally until the ORL merges with the lateral orbital thickening in the lateral canthal region. The levator labii superioris originates just below the orbicularis oculi muscle attachment to the medial orbital rim (Fig. 31.4). It is along the attachment of the orbicularis oculi muscle to the orbital rim that the tear trough deformity first manifests as a concavity that gets deeper with time. The tear trough deformity is at the inferior orbital rim most medially but very quickly falls below the rim, with the maximal distance from the rim occurring centrally. The hollowing can continue laterally in more advanced aging, presenting at or just below the orbital rim, where the retaining ligaments are thicker and less distensible.

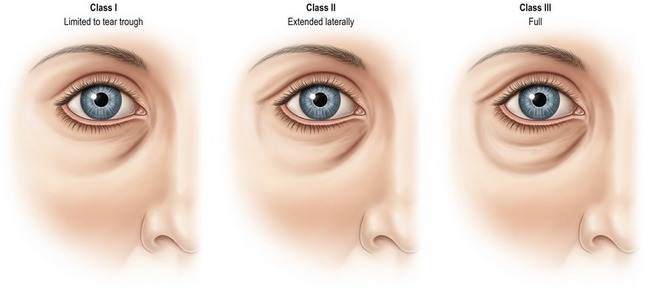
Clinically, the periorbital pattern of volume loss is categorized into three classes. Class I is limited to the tear trough or medial orbit. These patients sometimes show very mild flattening of the central area along the orbital rim in a reverse triangular pattern. Class II patients exhibit volume loss laterally as well as medially and they may have mild volume deficiency in the medial cheek and mild flattening of the central triangle. Class III patients exhibit a depression circumferentially along the orbital rim in a full and continuous pattern of hollowing medially to laterally (Fig. 31.5). This pattern is often associated with more advanced volume deficiency in the medial cheek, central reverse triangle, and malar eminence as well as demonstrating an oblique cheek crease highlighting the malar bags superiorly. The depth of the tear trough is used to estimate the volume required for correction with injections. Deeper and more extended patterns of volume loss (Classes II and III) can be associated with relative medial cheek/midface flattening, malar volume loss, as well as possible volume loss in the temporal region, brow and lower face.