| Reconstruction of skin defect at lateral canthus from trauma or after removal of carcinoma |
| Size and dimensions of defect |
| Age of patient |
| Eyelid and skin laxity, entropion, ectropion and lagophthalmos |
| Prior eyelid, facial surgery, trauma or skin cancers |
Introduction
Cutaneous defects at the lateral canthus often result from removal of neoplasms such as basal cell and squamous cell carcinomas. There are a multitude of different options to close large defects at the lateral canthus and the choice depends on factors such as the size of the defect, involvement of the eyelid margin, patient’s skin laxity, age, and surgeon’s preference. A balance between achieving form and function should be always considered.
If an upper and/or lower eyelid margin defect is present, attention should first be directed towards posterior lamellar reconstruction. This can be achieved with a periosteal flap ( Chapter 38 ), tarsoconjunctival flap ( Chapter 40 ), hard palate ( Chapter 36 ) or free tarsal graft ( Chapter 43 ). The anterior lamellar reconstruction can consist of adjacent tissue transfer or a free skin graft ( Chapter 27 ). The important principle to keep in mind is that one of the lamellae should be pedicle-based and a free graft should not be placed onto another free graft.
Although skin grafting can be used to close almost any anterior lamellar defect, adjacent tissue transfer is our first preferred option. Skin grafts must be thinned and the recipient site often has a palpable and visual step off owing to lack of subcutaneous tissue and muscle. Color and texture match, as well as graft survival, are other factors to consider with skin grafting.
Several options for adjacent tissue transfer at the lateral canthus are available, including a semicircular flap ( Chapter 39 ), Mustardé rotational flap ( Chapter 41 ) and a Limberg or rhomboid flap. At the lateral canthus, the lines of maximal extensibility (LMEs) and relaxed skin tension lines (RSTLs) are dictated by contraction of the orbicularis oculi muscle ( Chapter 1 ). Use of the rhomboid flap for lateral canthal defects places more tension on the horizontal meridians, and minimizes vertical traction forces that may result in anterior lamellar deficits, while blending the incisions laterally along the RSTLs to maximize the aesthetic outcome.
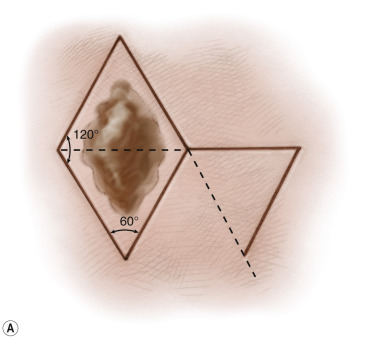
The optimal angles of the rhomboid are 60 and 120° to allow minimal wound tension upon closure ( Figure 42.1 ). If the area to be closed is not a pure rhomboid, the edges can be trimmed to convert the defect into a rhombic configuration. However, we prefer to minimize removal of normal tissue until the flap has been advanced and to remove any standing defects at the time of skin closure. The rhomboid flap can be applied at both the lateral and medial canthi for a satisfactory functional and aesthetic outcome.
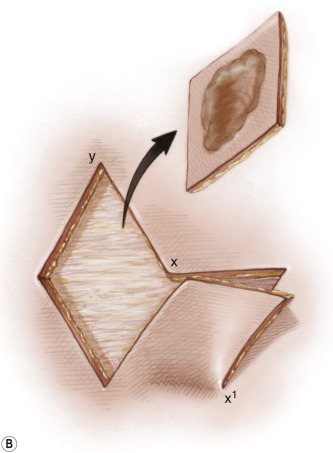
Surgical Technique