- •
Laser-assisted lipolysis is an effective procedure for localized adipose removal that may also induce simultaneous skin tightening
- •
The mechanism of action of laser-assisted lipolysis includes photo-acoustic, photomechanical, and photothermal effects
- •
Fibrous areas, previously treated areas, and areas of fat accumulation that have overlying skin laxity are some examples of areas amenable to laser-assisted liposuction
Introduction
Since its inception, lipoplasty, or liposuction, has continued to evolve with the addition of ultrasound-assisted, power-assisted, and then laser-assisted liposuction.
Since its approval by the Food and Drug Administration (FDA) in 2006, laser-assisted lipolysis (LAL) has become an integral tool used by many surgeons for simultaneous adipose removal and tissue tightening in selected patients. According to the Cosmetic Surgery National Data Bank, in 2010 liposuction of all types was the second most common cosmetic surgical procedure, with an estimated 289 016 cases, an increase of 63.4% from 1997. Liposuction was the most common cosmetic surgical procedure performed in men in 2010, and it was also the most common surgical procedure in the 35- to 50-year-old age category.
The evolution of liposuction has mirrored the desire to improve upon the standard. In the context of patient demand for improved results, shorter downtime, and fewer adverse events, LAL offers flexibility, in that the laser can be utilized solely to destroy adipocytes or can be used in combination with more traditional liposuction techniques. While true LAL is indeed an invasive procedure, the use of the laser alone or as an adjuvant to traditional liposuction has been purported to reduce blood loss due to coagulation of blood vessels, faster healing time, and less patient downtime.
Evolution and mechanism of action
The laser–tissue interaction occurring in LAL is based on the well-established mechanism of selective photothermolysis, described by Anderson et al. ; here the chromophores are adipose tissue and water.
Chromophores targeted in laser-assisted liposuction include adipose tissue and water
Apfelberg was the first to conduct trials utilizing LAL. Initial experiments were with a 40 W, 0.2 second pulse duration, 600 µm diameter Nd:YAG fiber that was housed in a 4–6 mm cannula. The fiber was not in direct contact with the fatty tissue and early findings suggested that this technique decreased patient pain, edema, postoperative bruising, and edema. A pulsed, 1064 nm Nd:YAG laser transmitted by an optical fiber, housed within a 1 mm cannula, which came into direct contact with adipose tissue, was then tried. It was reported that adipocyte lysis resulted directly from the laser energy. It was also concluded that the procedure had other beneficial effects compared with traditional liposuction, as further demonstrated by Badin and colleagues, who showed LAL decreased intraoperative blood loss and postoperative ecchymoses, and improved skin tightening. Of clinical significance was the observation that LAL was associated with stimulation of neocollagenesis in the dermal layer and dermal–adipose interface. This was believed to account for the purported cutaneous tightening and improved skin redraping seen postoperatively. Ichikawa and colleagues found that adipose cells directly treated with a 1064 nm Nd:YAG laser demonstrated greater histologic evidence of injury than nonlaser-irradiated adipose tissue that had been suctioned, and that laser treatment was associated with dose-dependent adipose lysis, and collagen fiber coagulation.
So as to improve results associated with LAL and to prevent collateral thermal damage, multiple wavelengths have been employed based on their preferential absorption by adipose and water compared with 1064 nm ( Table 10.1 ). Compared with a 1064 nm wavelength, a 1440 nm wavelength demonstrates greater fat absorption with less tissue penetration and scatter. This may be warranted in certain delicate areas where collateral thermal damage can lead to a higher risk of scarring.
| Wavelength | Adipose | Water |
|---|---|---|
| 1064 nm | 1 | 1 |
| 924 nm | 2.8 | 1.4 |
| 980 nm | 1.7 | 3.6 |
| 1320 nm | 5.9 | 11.5 |
| 1440 nm | 127 | 252 |
Mordon et al. utilized a continuous-wave 980 nm diode laser (Pharaon®, Osyris, Hellemmes, France) to target adipose. Evidence of carbonization within the adipose tissue and collagen fibers was detected, which was thought to be due to a combination of the higher laser fluence and continuous waveform. It may be therefore deduced that a pulsed wave laser with shorter pulse duration would allow for the thermal relaxation of the target chromophore and therefore less collateral thermal destruction.
The preferential absorption of laser energy by adipocytes causes deformation of the adipocyte and volume expansion leading to cell lysis. The adipocytes that are closest to the laser fiber tip are exposed to the highest fluence and undergo photo-acoustic/photomechanical destruction. Surrounding adipocytes are exposed to lesser fluences and are therefore subject to more photothermal-based damage. This may result in cellular changes but not necessarily immediate cell lysis. The immediately destroyed adipocytes as well as the thermally injured cells, which may eventually lyse, are the damaged adipocytes which are theorized to be undergoing apoptosis and eventual removal by phagocytosis, possibly via activated macrophages.
Additionally, salutary effects of LAL such as decreased postoperative blood loss may be due to the absorption of energy by oxyhemoglobin and methemoglobin. The 1064 nm device has absorption peaks for both chromophores, with methemoglobin being preferred, possibly accounting for the coagulation effects seen. The theorized associated end benefit of LAL is the effect on skin tightening and redraping. This is thought to be due to a photostimulatory effect due to the collateral thermal energy acting upon dermal and adipose collagen. Lower energy levels farther away from the laser tip are sufficient to cause thermal heating but not complete destruction of collagen.
The photothermal effects of LAL, like those of any laser procedure, must not be underestimated. Bulk heating in any one location can produce deleterious effects. This can include thermal burns and cutaneous necrosis. Empirical findings suggest that an internal temperature between 48 °C and 50 °C must be reached for collagen denaturation and subsequent skin tightening, and therefore many new devices are being equipped with an internal temperature gauge to cease laser firing if the temperature at the fiber tip exceeds a corresponding threshold. External temperatures between 38 °C and 41 °C have been identified as safe and efficacious. This skin surface temperature can also be monitored with the use of an external infrared thermal probe.
Patient selection
With any elective cosmetic procedure, patient selection and patient education are key components to a successful outcome. Patient selection and consultation start as soon as a patient expresses interest in the procedure. Patients may vary in their degree of knowledge of ‘laser lipolysis’. Some patients may expect an external laser device, and not an invasive procedure, so it is important to understand the base knowledge and expectations of each patient. The educational process can be initiated when a patient calls the office inquiring about the procedure or, via a patient questionnaire when a patient presents for the initial consultation. The more informed and realistic the patient expectations, the more ‘successful’ the procedure will be.
Indications
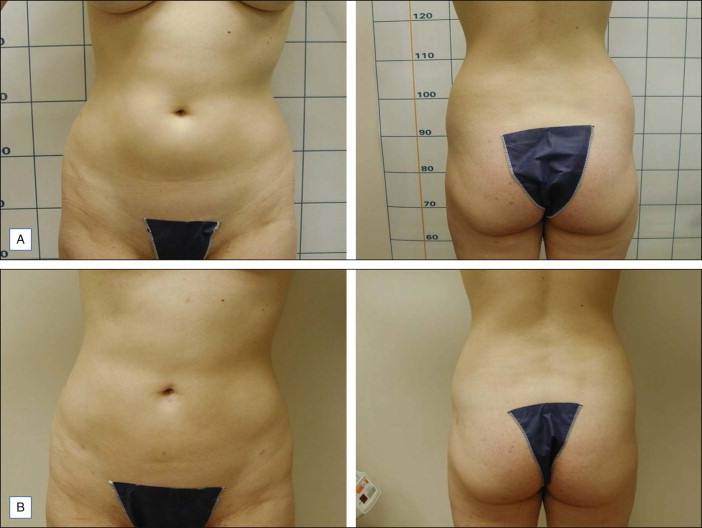
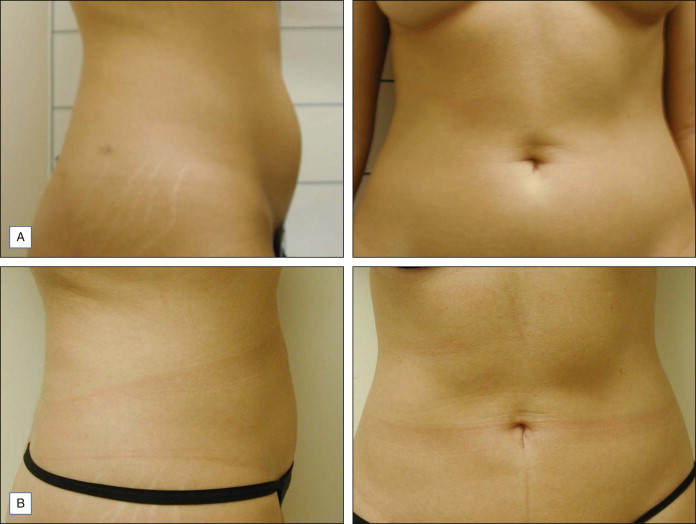
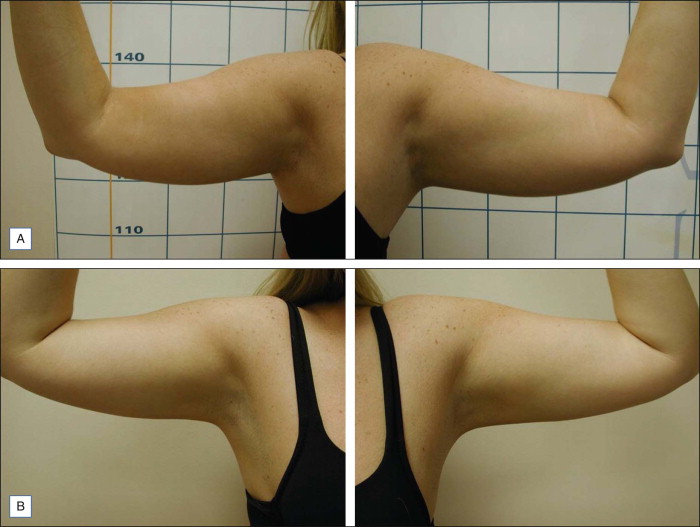
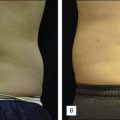
LAL is indicated for the localized destruction of adipose tissue as well as skin tightening, with the latter effect distinguishing it from traditional liposuction. Areas in which LAL has been used effectively include the abdomen ( Figs 10.1 and 10.2 ), flanks ( Fig. 10.1 ), upper arms ( Fig. 10.3 ), submental/neck area ( Fig. 10.4 ), back, inner and outer thighs, knees, calves, and ankles. LAL may also be suitable for patients who have had previous procedures such as traditional liposuction.
Laser lipolysis with or without subsequent aspiration of fat can be useful for areas of recalcitrant adiposity remaining after previous procedures.

Fibrous adipose tissue areas are commonly encountered in areas such as the male breast, hips, and particularly the back. Due to the fibrous elements at these sites, these areas may be responsive to LAL, which can release fat encased fibrous tissue with decreased trauma. Also, since a relatively smaller cannula size can be used during LAL, trauma may be mitigated compared with the use of larger cannula sizes typically needed for traditional liposuction. LAL has also been used to remove lipomas.
Patient evaluation
As with traditional liposuction, real time patient evaluation and examination are crucial to understanding patient concerns and expectations prior to LAL. Realistic expectations regarding the timeline of events, postoperative care required, degree of fat removal, and degree of tissue tightening can also be conveyed at this juncture. Patients may physically highlight their areas of concern, as their linguistic representations may be inaccurate. For instance, when a patient refers to the ‘flank area’, he or she may in fact be thinking of a different anatomical location. Patients may also be made aware of fat pockets in contiguous regions that may require additional treatment to achieve the best overall results; for example, focal LAL of the lower abdomen may leave a patient with a full, overhanging, upper abdomen.
Topics that should emphasized during the consultation in addition to routine preoperative screening include postoperative care and bruising, degree of fat removal, time to see full results (3–6 months), and realistic expectations of skin tightening.
Preoperatively, a thorough medical, surgical, medication, and allergy history should be obtained. Over-the-counter and herbal medications should also be considered. Many of these medications can interact with the metabolization of tumescent anesthesia through activation or inhibition of cytochrome P450 enzymes. Medications that are contraindicated include warfarin, clopidogrel bisulfate, aspirin, nonsteroidal anti-inflammatory drugs, and other anticoagulants, as these will increase the risk of bleeding and hematoma formation. Pregnancy or lactation are also contraindications.
The ideal candidate would be someone who is in good health, maintains a healthy diet, enjoys stable weight, and exercises regularly. In the context of LAL, a healthy patient is generally an American Society of Anesthesiologists’ Physical Status Classification System class I or II, that is, either ‘normal healthy patient’, or ‘mild system disease and no functional limitation’, respectively. Requesting medical clearance may be appropriate for patients over 60 years of age and those who have a history of cardiovascular disease, hypertension, or diabetes.
Patient evaluation checklist
- ▪
Past medical history: highlight clotting or bleeding disorders, liver disease
- ▪
Past surgical history – related to the area being treated, including pre-existing scars
- ▪
Medication use/drug allergies
- ▪
Physical exam: standing position
- ▪
Diet history
- ▪
Baseline body weights
- ▪
Circumference of area of interest
- ▪
Body mass index (BMI)
- ▪
Baseline images
- ▪
Consent forms
- ▪
Baseline blood laboratories: complete metabolic profile, complete blood count with platelet count, liver function tests, prothrombin and partial thromboplastin time, hepatitis B/C serologies, human immunodeficiency virus serologies, beta-human chorionic gonadotropin pre-surgery/urine pregnancy test the day of surgery
It is important to note any bleeding problems or infections in the past as well any previous surgical or noninvasive procedures. Asking about previous scars can help ascertain how a patient heals and can elicit any previous surgical procedures.
Physical exam
The physical exam may be performed with the patient standing to assess for baseline irregularities and asymmetry. Asymmetries should be noted, highlighted, and explained to the patient, who may or may not be aware of such. The patient should be either completely undressed or given a disposable bikini undergarment, which has no elastic constriction. This avoids any distortion of the natural contour of the area and any artifactual step-offs when evaluating the patient. The pinch test, which is done by pinching the area of interest between the thumb and index finger, is often used both pre-surgically and during the operation. An area of adiposity where the surgeon can pinch at least an inch suggests an area where LAL can be effectively performed. A pinch of less than one inch may indicate lack of sufficient fat to suction and increased risk of postoperative irregularities.
Baseline body weight as well as calculated BMI may be recorded. It is important to inform the patient that these parameters may not change post-procedure since liposuction is not a weight-reducing procedure. Circumferential measurements of the area being evaluated (bilateral thighs, hips, or waist) may be more likely to change post-procedure.
Skin laxity may also be assessed during the physical exam as this can be targeted and improved by LAL. Though it may tighten the dermal layer and therefore improve skin tone, LAL may not be able to create a completely flat, washboard appearance, which some patients may be expecting. To assess skin elasticity, the surgeon can perform the ‘snap test’ where the skin is gently pinched between the thumb and the index finger and then released. If there is an instantaneous recoil to rest position, this indicates good elasticity, and therefore a favorable potential response to LAL. If, however, there is slow recoil or no recoil at all, this indicates poor elasticity. Such patients may be made aware that they may be more likely to have residual skin folds after LAL. Other indications that textural skin abnormalities or incomplete skin retraction may be post-procedure problems include the preoperative presence of cellulitic areas, dimples, larger depressions, excessive striae, and inelastic hanging skin folds.
Baseline photography
Appropriate imaging pre-treatment facilitates gauging improvement post-treatment as patients and physicians may not recall pre-surgical conditions many months later. Photography and imaging of adiposities can be easily altered by angle, lighting and shadowing, therefore these parameters are ideally standardized. Having a uniform background, fixing the patient position, and keeping constant the distance at which the image is taken can make for excellent quality images. Overhead or tangential illumination of the areas may be used to better visualize the surface area. Photographs may be taken with the patient standing and muscles relaxed. A total body photograph as well as multiple close-up photos of the individual areas can be obtained at the same time, with the former placing the latter in context. Subsequently, and before surgery, these images can be shown to the patient in order to initiate a frank discussion about the outcomes that are realistically possible.
Use a standard black background for taking all photos. This will help to standardize images.
Use standard paper undergarments when taking photos to avoid distortion by waistbands and elastic banding.
Another option for imaging is a three-dimensional imaging system. While not necessary and inherently more costly, this technology can dramatically highlight post-procedure changes. The technology uses stereo-paired cameras to map out surface features. This technique is more resistant to inadvertent subject movement and also partially negates the effects of ambient room lightening. The imaging software additionally calculates the surface height and volume change within the treatment area.
Treatment course
LAL is performed in a manner similar to traditional or power-assisted liposuction and preparation can likewise be quite similar. Informed consent is obtained before commencement. A urine pregnancy test may be performed on the day of surgery to confirm that the patient is not pregnant. Some physicians may prefer to dose oral antibiotics 24 hours before or at the time of tumescent infusion. The antibiotic is routinely one that covers the most common contaminating pathogen, Staphylococcus aureus . Some physicians offer the patient oral lorazepam 1–2 mg, or diazepam 5–10 mg at the time of surgery; in some instances, oral clonidine 0.1 mg on the day of the procedure may be administered if the patient’s blood pressure is stable and above 100/70 mmHg in order to prevent epinephrine-induced tachycardia.
LAL is typically performed under local tumescent anesthesia alone, or supplemented with intravenous sedation, intramuscular pain medication, or epidural block. Some physicians perform a modified version of the procedure under general anesthesia.
Once marked, the patient is brought to the operating room or surgical suite and prepped widely, with the sterile area encompassing the surgical site area and proceeding well beyond to avoid inadvertent contamination. Usually either Betadine® (Becton Dickinson, Franklin Lakes, NJ) or Hibiclens® (Regent Medical, Norcross, GA) is the prep chemical. Skin cleansing is often done with the patient in the standing position. The patient may then be placed on the operating table upon the sterile draping. External pneumatic compression devices such as Venodyne® (Columbus, Mississippi) are occasionally also used on the legs, but this is not common or required.
Entry points are made in well-selected positions that provide overlapping access to the treatment site, and are also ergonomically positioned for optimal hand-positioning during treatment. The precise selection of sites is contingent on the area being treated. Multiple small entry points are typically favored over fewer larger diameter entry sites. This approach allows for suctioning of a given area from multiple points, thus allowing a smooth final contour, and smaller entry points also heal more quickly and less noticeably. A small #11 blade incision can be used to create entry points. Alternatively, a 1.5 mm or 2 mm punch biopsy tool may be employed, and it has been suggested that the resulting small wounds may heal particularly well ( Fig. 10.1 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


