Historical Perspectives
Hair removal is one of the most common cosmetic procedures performed today. In 2009, industry revenue for hair removal, either personally or by a practitioner, totaled approximately $244 million. It has been practiced since prehistoric times with specific modifications due to local cultural, religious, as well as personal aesthetic preferences. Ancient Egyptian men shaved hair from their heads and faces to prevent grasping during battle; women in the Middle Ages plucked and shaved hair on their eyebrows and anterior hairline to conform to contemporary standards of beauty.1 Contemporary demand ranges from cases of hirsutism and hypertrichosis to normally distributed body hair that is unwanted. Hirsutism is abnormal hair growth in women in androgen-dependent sites, whereas hypertrichosis is excess hair growth in a body site (anywhere on the body) independent of hormones.
Depilation, the removal of the hair shaft, and epilation, the removal of the hair shaft and bulb, are the two primary methods of hair removal. Shaving is an example of depilation, whereas epilation includes methods such as waxing, electrolysis, and laser hair removal. Epilation hair removal provides results that usually last about 8 weeks; depilation results only last for approximately 2 weeks.2
Shaving, an extremely cost-efficient and popular method for men’s facial hair and women’s legs and underarms, does not alter the hair cycle and is a temporary solution to hair growth.3 Historically, shaving tools have ranged from sharpened animal teeth and flint to modern electric and nonelectric blades.
Waxing, which has existed since ancient times, provides temporary hair removal and can treat large areas efficiently, albeit at a risk of skin irritation and pain.4 Electrolysis results in potentially permanent hair removal by a probe passing an electrical current to destroy the hair follicle. It is however a slow and operator-dependent method with wide-ranging rates of complications such as scars and pigment changes.5 Laser hair removal utilizes the existing melanin in hair follicles for specific targeting called selective photothermolysis. It is important to appreciate the evolution of hair removal because it guides providers about needs for future improvements as well as motivation for patient demands.6
15.2 Hair Follicle Growth and Anatomy
The hair follicle is a hormonally active structure with specifically programmed growth. It can be divided into three anatomical portions from superficial to deep: infundibulum, isthmus, and inferior segment (▶ Fig. 15.1). The inferior segment is bordered inferiorly by the base of the follicle and extends superiorly to the erector pili muscle. The isthmus extends from the erector pili muscle to the sebaceous gland duct. The infundibulum extends superiorly to the follicular orifice. The dermal papilla supplies proliferating cells at the base of the follicle. Melanocytes, located near the infundibulum, provide the pigment that determines hair color.
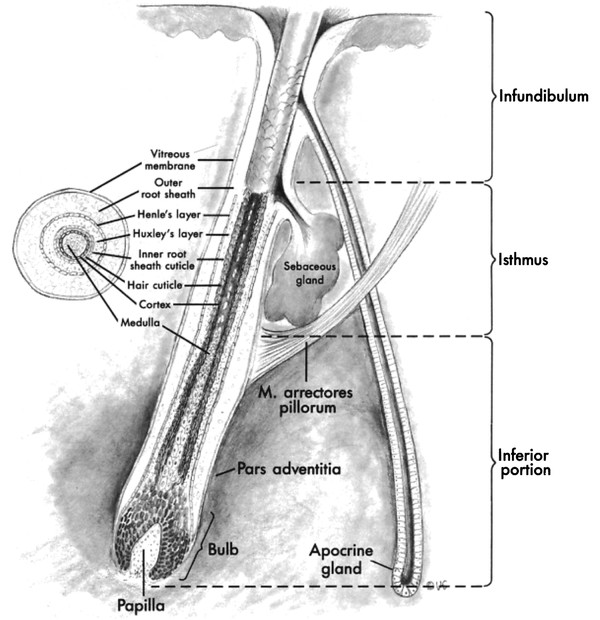
Fig. 15.1 Hair follicle anatomy. The hair follicle can be divided into three anatomical portions from superficial to deep: infundibulum, isthmus, and inferior segment. The inferior segment is bordered inferiorly by the base of the follicle and extends superiorly to the erector pili muscle. The isthmus extends from the erector pili muscle to the sebaceous gland duct. The infundibulum extends superiorly to the follicular orifice. The dermal papilla supplies proliferating cells at the base of the follicle. (Reproduced with permission from Papel I. Facial Plastic and Reconstructive Surgery. 3rd ed. New York, NY: Thieme Medical Publishers; 2009.)
The hair follicle can be in any one of three different metabolic phases: anagen, catagen, and telogen. Anagen is a period of active growth; catagen involves degradation through apoptosis. Telogen is a resting phase and the relative length of each phase is body-site dependent, although at any given time 90% of the body’s hair is in the anagen phase. The follicle can produce various types of hair. Lanugo hairs are found on a fetus and lost during the neonatal period. Vellus hairs have a diameter of 30 µm and are the most prevalent hairs in the body, whereas terminal hairs are much thicker at 300 µm and more ideally suited for laser hair removal.
15.3 Mechanism of Laser Hair Removal
Laser light is unique in that it has one specific wavelength (monochromatic), its rays are parallel (collimated), the rays are in phase with each other (coherent), and are of high intensity. Light from lasers is scattered, transmitted, reflected, or absorbed by the skin surface. Chromophores such as melanin absorb light energy that is in the red or infrared range of electromagnetic radiation (600–1,100 nm). Selective photothermolysis is dependent on the heating and subsequent destruction of the chromophore without collateral damage to surrounding tissue. As described earlier, in the hair follicle there is spatial separation between the location of melanin near the infundibulum and the deeper stem cells. As melanin absorbs the light energy and converts it to heat, the deeper stem cells are thermally injured. The amount of heat absorbed at a given wavelength is determined by the energy density (fluence, measured in joules [J/cm2]) and the length of time at a given temperature (pulse duration). Selectivity occurs when pulse duration approaches the thermal relaxation time, the time necessary for tissue to cool to half its peak temperature. Therefore, long-pulsed lasers work well if they approach the thermal relaxation time of hair follicles, which is between 10 and 100 ms.7 Spot size is also an important variable. Due to the phenomenon of lateral scattering of light once it penetrates the skin, the spot size has an effect on the effective depth of light penetration. If all other variables are held constant, a larger spot size will result in an overall greater depth of effect, which is desirable for targeting hair follicles.
The hair in melanin competes with epidermal melanin, increasing the risk of collateral damage in darker skinned individuals. With lighter colored hair, not enough energy may reach the hair follicle stem cells to cause thermal damage. Therefore, the ideal candidate for laser hair removal has light skin and dark hair.
15.4 Types of Lasers
The types of lasers commonly used for hair removal include ruby, alexandrite, diode, and the neodymium:yttrium aluminum garnet (Nd:YAG) (▶ Table 15.1). Wavelengths of these lasers range from 694 to 1,064 nm. In general, lasers with longer wavelengths are less absorbed by epidermal melanin and have less tissue side effects.8 Often the intense pulsed light (IPL) device is grouped with laser hair removal instruments but the emission is rather different. Laser light is monochromatic (single wavelength) and has very slight divergence, whereas the IPL device emits light along a range of wavelengths that is noncoherent. The advantages of the IPL mechanism are its low cost and ability to treat large areas; however, more treatments may be required to achieve the same efficacy as compared to the other lasers mentioned. Electro-optical synergy (ELOS) technology combines the benefits of both radiofrequency and IPL technologies for hair removal. The light (optical) component heats the hair follicle, while the radiofrequency modality (electrical) focuses the heat on the hair shaft. This dual treatment system can be used for all skin types since melanin is not targeted.
Laser | Wavelength (nm) | Fitzpatrick skin type |
Long-pulsed ruby | 694 | I and II |
Alexandrite | 755 | I–III |
Diode | 810 | III–V |
Neodymium:yttrium aluminum garnet (Nd:YAG) | 1,064 | IV–VI |
The long-pulsed ruby laser, which has a wavelength of 694 nm, was approved for hair removal by the Food and Drug Administration (FDA) in 1997 and is effective in treating lighter skinned individuals.9 The alexandrite laser has a wavelength of 755 nm, and long-term efficacy with long-pulsed alexandrite lasers has been as high as 80.6%. Lloyd and Mirkov10 studied 11 patients receiving five alexandrite laser treatments to the right groin at 3-week intervals with no evidence of scarring or pigment changes. This procedure is recommended for Fitzpatrick skin types I to III because of reduced competition with epidermal melanin. Lasers with longer wavelengths are less absorbed by epidermal melanin and have less tissue side effects.8 The diode laser has a wavelength of 810 nm and can be used for slightly darker skin types. The FDA recently approved a diode laser for home use.11 Such devices offer greater privacy and convenience for the patient and appear to be both safe and effective.12
The Nd:YAG laser (1,064 nm) can be used for virtually all skin types. The longer wavelength will penetrate deeper into the skin, while leaving the epidermis undamaged. Although longer wavelength lasers have less side effects in darker skinned individuals, comparisons of efficacy among the different lasers have shown varying results. Chan et al13 studied 15 Chinese women for mainly axillary hair removal with diode laser on one side and Nd:YAG on the other with 36 weeks of follow-up. Nd:YAG laser treatment was associated with greater immediate postprocedure pain; however, both laser treatments showed similar efficacy with regrowth rates approximately 20% at 6 weeks. Li et al14 also studied axillary hair removal comparing the efficacy of the diode and Nd:YAG lasers. In their study, 29 Chinese women received three treatments at 4-week intervals. At 8 weeks, there was a higher rate of hair reduction and less postprocedure pain associated with the diode laser side as compared to the Nd:YAG laser-treated side.
Cooling devices are also important to consider during laser hair removal because treatment can be quite painful. Cooling the epidermis not only diminishes pain and side effects at the treatment site, but also allows for the ability to use increased fluence at the procedure site. Cooling can be accomplished by circulating cold water or coolant in the laser handpiece, or applying external forced-air cooling.
15.5 Pretreatment Considerations
As in any treatment offered by a trained provider, a thorough medical history is necessary. Any history of endocrine or menstrual abnormalities, such as polycystic ovary syndrome, could signal a systemic cause for unwanted hair that can be treated medically. Active infection with the herpes simplex virus (HSV) in the area of desired treatment is a contraindication to treatment. If there is a history of HSV infection, prophylactic treatment with valacyclovir a day before treatment is recommended.15 Although rare now, gold-salt intake is a contraindication because it can cause cutaneous hyperpigmentation (chrysiasis).16 Active use of isotretinoin is also a contraindication due to impaired tissue healing and skin fragility.
Thorough patient counseling and consent are also important before laser hair removal treatment is initiated. A detailed consent that includes the complications associated with laser hair removal should be obtained (▶ Fig. 15.2). Patients with light-colored hair should be advised that they are poor candidates for laser hair removal. Because hair grows in cycles, laser hair reduction must be performed in a series of procedures, generally, approximately 6 to 8 treatment sessions about 3 to 8 weeks apart. Patients will notice fewer hairs regrow after each successive treatment session. Patients can expect a 10 to 25% hair reduction after each process. Once treatment end point has been reached, patients should understand that periodic touch-up procedures may be required; they will obtain hair reduction but not necessarily permanent hair removal.
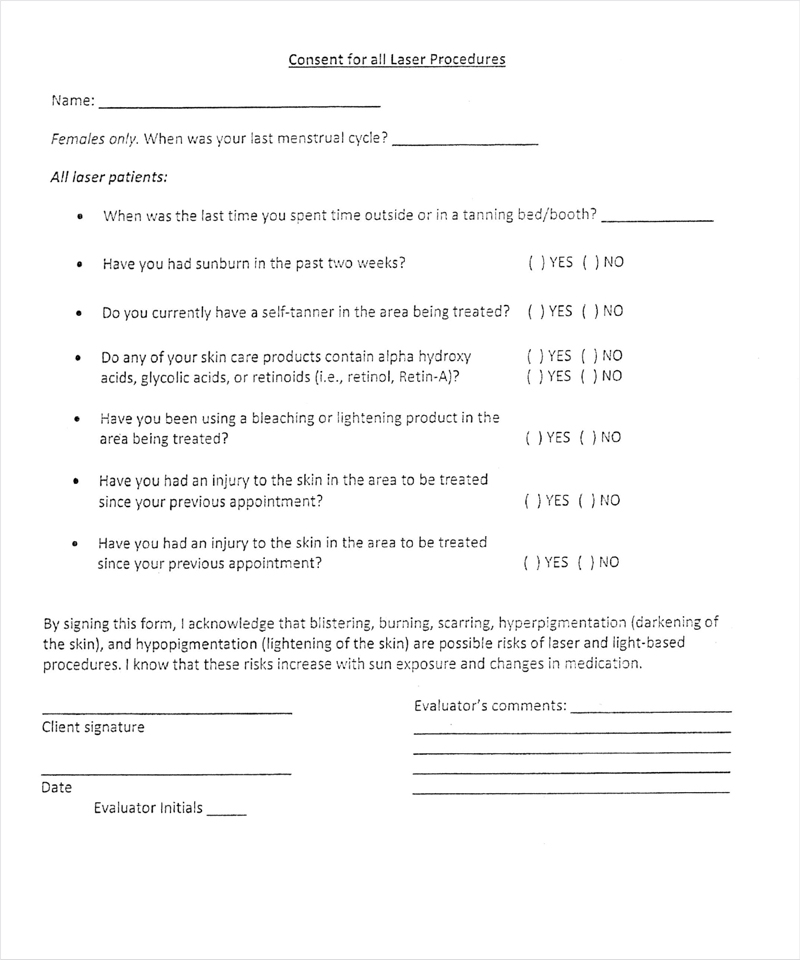
Fig. 15.2 A sample of an informed consent and preprocedure questionnaire for laser hair removal. (continued)
Related posts:
 Combining Different Lasers in the Same Session for Optimal Outcomes in Treating Aging Skin
Combining Different Lasers in the Same Session for Optimal Outcomes in Treating Aging Skin
 Treatment of Acne Rosacea
Treatment of Acne Rosacea
 Laser Solutions for Scar Management
Laser Solutions for Scar Management
 Enhanced Medium-Depth Chemical Peels
Enhanced Medium-Depth Chemical Peels
 Private: Lasers, Peels, and Abrasion Techniques for Latino Skin
Private: Lasers, Peels, and Abrasion Techniques for Latino Skin
 Private: Laser-Assisted Lower Lid Blepharoplasty
Private: Laser-Assisted Lower Lid Blepharoplasty



