Key points
- •
The cosmetic impact of acne impacts on up to 96% of patients.
- •
Laser and light source treatment represents an alternative approach to standard acne treatments.
- •
An understanding of the pathophysiology of acne leads to an understanding of device treatments of acne.
- •
Laser and light source treatments of acne can occur via pure photochemical, combined photothermal and photochemical, photosensitizer assisted photochemical and/or photothermal, and pure photothermal means.
Introduction
Acne vulgaris accounts for over 30% of all dermatology visits. It is also a common cause for visits to almost all physicians. It has been estimated that 70–96% of all individuals will suffer from acne vulgaris at some point in their lifetime. Recent evidence suggests that over 40 million American adolescents and 25 million American adults are affected by acne vulgaris. An increasing number of people seek acne laser or laser-like treatments as an alternative to taking systemic agents for their acne.
In its simplest form, acne vulgaris is a disorder of the sebaceous glands. Obstruction of the sebaceous glands leads to the production and proliferation of bacterial growth within the sebaceous glands. The bacteria most commonly associated with the formation of acne vulgaris is Propionobacterium acnes ( P. acnes ). Inflammatory acne presents with papules, pustules, and cysts.
It is through an understanding of the pathophysiology of acne that one can optimize light based treatment of this common problem. The sebaceous follicle clearly is the site of acne lesion development. The most superficial portion of the follicle, the acroinfundibulum, shows similar anatomy to that seen in the adjacent epidermis. Deposition of epidermal melanin, as seen in open comedones (blackheads), and the addition of ceramides to sebum, occurs here. Deeper into the infundibulum at approximately 200 µm is the infrainfundibulum. This is the site of initial comedogenesis. It is in this infrainfundibulum that various P. acnes . species activate chemotactic factors and pro-inflammatory mediators. Lipases, hyaluronidases, and proteases are among these compounds. Macrophages release cytokines and activate the complement pathway through various receptors. Changes in infundibular keratinization and inflammation follow their release. With these changes one begins to see the classic inflammatory papules and pustules of acne.
Further inferiorly, the infrainfundibulum splits into numerous sebaceous ducts which provide communication between the lobules of sebaceous glands and the infundibulum. ‘Hyperfunctioning’ sebaceous glands are one of the main contributors to acne. In acne patients, sebaceous glands and the entire sebaceous follicle are much larger than in their non-acne counterparts. Their miniaturization results in a marked decrease in acne lesions count and severity. Several lasers and laser-like devices may be effective because of their thermal impact on these structures.
Historically, there have been a large variety of effective medications to treat those individuals suffering from acne vulgaris. These include topical and systemic antibiotics, topical benzoyl peroxide, topical salicylic acid derivatives, and a variety of topical sulfa pre-parations. Topical and systemic retinoids round out the successful standard treatments for acne vulgaris. Despite continuing advances, there are drawbacks to each group of therapies.
Patient selection
Some of the topical medications are irritating and often not tolerated in colder environs. Most topical therapies are slow to achieve an acceptable onset of action, some requiring several months to become successful. Systemic antibiotics, the mainstay for inflammatory acne for many years, have recently been reported to show up to a 40% drug resistance with the commonly used oral tetracyclines, erythromycins, and sulfa derivatives. A recent report has even suggested that the long-term use of systemic antibiotics in women may be associated with a higher incidence of breast cancer.
Exposure to natural and artificial UV light has been reported to be successful in the treatment of acne vulgaris. Although the exact mechanism of action of ultraviolet light induced improvement of acne is not fully understood, it is felt to be due, in part, to destruction of P. acnes bacteria in the sebaceous unit. This natural endogenous photodynamic therapeutic (PDT) reaction clearly can lead to improvement in the treatment of acne vulgaris. However, UV light associated photodamage precludes this method as a mainstay of acne treatment.
Indications and avaiiable technolgies
Several lasers and laser-like devices are currently being utilized to treat acne. A variety of mechanisms of action explain the effect of these devices on acne. Such devices can be divided into groups whose effects are primarily (1) pure photochemical; (2) combined photothermal and photochemical; (3) photosensitizer assisted photochemical and/or photothermal; and (4) pure photothermal ( Table 8.1 ). These are described below.
| Category | Device | Device | ||
| Pure photochemical | Blue light | Red light | ||
| Combined photothermal and photochemical | Pulsed dye laser (pdl) | Intense pulsed light (ipl) | ||
| Photosensitizer assisted photochemical and/or photothermal | Ala + light/laser | |||
| Pure photothermal | 1319/1320 nm laser | 1450 nm laser | 1540 nm laser | Monopolar radiofrequency (rf) |
Results
Pure photochemical
Using low-level photochemistry requires either a continuous-output blue light source or longer wavelength visible light sources, These systems typically involve pan-facial treatment with multiple banks of lights ( Figure 8.1 ). Photochemical treatment of acne using endogenous porphyrins is based on the principle of light-based P. acnes photoinactivation. P. acnes produces coproporphyrins and protoporphyrins. Most of the natural reddish-orange fluorescence seen on the face, under 365 nm light is due to the coproporphyrin III produced by P. acnes . The intercellular porphyrin stores will, under long wave UVA and certain visible light wavelengths, cause cell killing through membrane damage. This PDT effect has been demonstrated in vitro. However, the efficiency of bacterial killing with endogenous porphyrins is low, and consecutive in-vitro illuminations are necessary to reduce viability by four or five orders of magnitude.
Nevertheless, the treatment of inflammatory acne vulgaris with P. acnes destroying blue light sources has been extensively evaluated. reported that after treatment with a blue light source, 63% of inflammatory lesions responded while 45% of comedomal lesions were also improved. Kawada also showed that 65% of inflammatory acne lesions responded to blue light therapy. Finally, Elman & Lebzelter have shown 60–75% improvement with a newer high-intensity blue light source. Finally, Gold also reported his findings with a blue light source in 40 individuals with mild to moderate inflammatory acne vulgaris. Treatments were conducted twice a week for 4 weeks, with follow-up at 1 and 4 months. The results of this trial showed a 43% improvement in inflammatory acne. Another blue light source has also been shown to be more effective than topical 1% clindamycin solution in treating inflammatory acne vulgaris during a four week treatment period. Most clinical trials have evaluated two treatments per week for 4 weeks with only 1 and 3 month follow-up evaluations. Unfortunately, most clinical trials also show, on average, a 20% non-responder rate.
Recently the focus in acne therapy has been on blue–violet light continuous wave (CW) sources. These devices emit light in the 25–100 mW/cm 2 range, use exposure times of 10–20 min, and are painless. As described above, it is thought that endogenous porphyrins (produced as byproducts of P. acnes metabolism) are excited and singlet oxygen is formed. With these devices, the results have also been variable and the endurance of endogenous porphyrin based treatment (with power densities of <100 mW/cm 2 ) has not been well defined. In one study, 34 patients were treated with a blue light device. Patients were divided into two groups (based on high versus low dose) and treated with a high-energy high-pressure blue light (400–420 nm). After 10 of 20 treatments, performed four times per week for 5 weeks, there was noted acne improvement. The total light dose in the larger group was 650 J/cm 2 . Interestingly, improvement did not increase between 10 and 20 treatments. Also, the lower dose group showed greater improvement.
In this study, subjects were not followed past the last treatment. In another study, 107 patients were randomized into four treatment groups: blue light, blue–red light, cool white light, and benzoyl peroxide. Treatment sessions lasted 15 mins and the cumulative doses over 12 weeks of daily treatments were 320 J/cm 2 for the blue light and 202 J/cm 2 for red light. White light was used as a control. Overall, the blue–red light combination was superior, showing 75% reduction in inflammatory lesions after 12 weeks. The blue light and benzoyl peroxide produced similar improvement of about 60% after 12 weeks. Low output white light (a room light ‘control’) was associated with a 25% decrease in counts.
Goldberg et al treated 24 patients with symmetrical facial acne with twice weekly treatments with the combined 415 and 633 nm LED treatments. There were 4 weeks of treatments, and the final evaluation was 4 weeks after the final session. Mean lesion count reduction was 46%. At the 12 week follow-up, reduction was 81%. Goldberg conceded that LED treatments, although painless, might not be enough alone to be effective. Finally, in another similarly designed study from Korea, reduction in inflammatory lesions was 78%, 8 weeks after the final treatment.
In another study, patients were treated three times per week for a total of 20 sessions. Treatments required about 20 min. Three types of light were used: (1) ‘full spectrum’, a mix of UVA, violet and green light (2) ‘violet light’, a mix of UVA and violet light with a small contribution of green light, and (3) ‘green light’, a mix of mostly green light with a small contribution of violet light. The investigators observed a final reduction of acne severity of 14%, 30%, and 22% at the end of 20 sessions with full spectrum, violet, and green light respectively. Overall, the violet light group did best, but the differences were not significant. As in most studies, the light effects were primarily on inflammatory lesions, with little effect on comedones and papules. Kawada et al treated 30 patients using a blue light source, which has a peak emission between 407 and 420 nm. The irradiance was 90 mW/cm 2 , with two treatments per week for up to 5 weeks. There was an overall 55% reduction in the number of lesions (all types). Seventy seven percent of patients showed either improvement or marked improvement with 20% either worsening or remaining unchanged. One month after the final treatment most of the improvement was sustained.
Combined photothermal and photochemical approach
The visible light devices described above work exclusively through photochemical mechanisms. That is, singlet O 2 production by an endogenous PDT reaction results in P. acnes destruction. The visible light induced irradiances are insufficient to achieve significant temperature elevations. The following studies involve irradiances where there is some degree of temperature elevation, as well as a possible PDT-mediated antibacterial effect.
Seaton et al examined the effects of low fluence pulsed dye laser (PDL) treatment in the treatment of acne. They found that acne severity improved markedly versus controls (53% lesion count decreases in treatment areas versus only 9% in controls). There was no difference between the high and low fluence treatment groups. Another study found that the PDL at purpuric pulsewidths can improve inflammatory acne. Thirty patients were treated with low fluence PDL every 4 weeks (total of three sessions) and evaluated 12 weeks after the final treatment. They noted a 57% reduction in inflammatory lesions but just a 27% decrease in comedones.
The role for low fluence PDL has been somewhat controversial, as using similar laser settings as Seaton et al, were unable to show statistically significant reduction in lesion counts in a split-face study. They performed one or two treatments and followed the patients 12 weeks later. More recently, Chu (the senior author from the Seaton study) countered by noting the small number of patients in the Orringer study. Further studies are required to analyze the role of the PDL in the treatment of acne. Most intense pulsed light (IPL) devices emit in the 500–1200 nm range, with the greatest portion of the spectrum in the 530–700 range. IPLs have been used in two scenarios, the first using higher settings normally applied for rosacea and photorejuvenation. These settings, with or without topically applied ALA, are able to achieve sufficient heating of telangiectasia and pigment dyschromias to diminish their appearance.
Published studies of IPL with ‘high’ fluences (without ALA) have shown a reduction in redness and acneform papules. A recent report of an IPL equipped with a 530–750 nm filter showed improvement in reducing acne red macules but did not affect inflammatory acne. Traditional light doses for telangiectasia reduction were applied. In another scenario, lesser settings are used with multiple pulses. In this second approach type, lower settings presumably will change the ratio in favor of photochemical over photothermal mechanisms. There are newer pulsed light sources that use low energies and a spectrum that allows for considerable violet–blue and/or green–yellow–red light emission. Dierickx, using this system, with both violet and green light handpieces, found significant clearing of lesions (after up to five treatments over 5–15 weeks). Follow up to 3–6 months resulted in only a partial return of lesion counts in most patients.
A variety of intense pulsed light sources (IPLs) have been used for the treatment of acne vulgaris. The IPL induced mechanism of action would appear to be similar to that seen with blue light therapy. In one IPL study, 85% of patients showed greater than 50% improvement in their acne lesions. Up to 20% of the patients were non-responders.
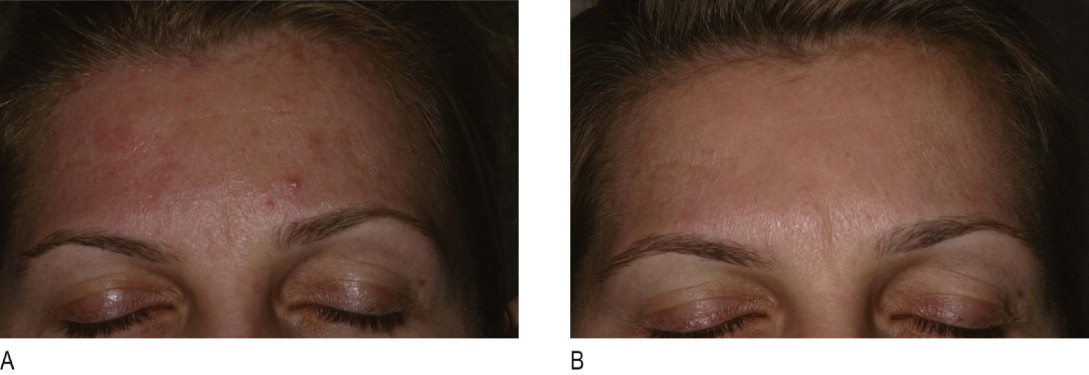
Photosensitizer assisted photochemical and/or photothermal approaches
When pre-treated with topical ALA (a pro-drug that creates PPIX), P. acnes produces more porphyrins than is normally produced. In this case, the bacteria are inactivated by several orders of magnitude more than without ALA. On the other hand, a recent study showed no decrease in surface P. acnes counts after red light ALA PDT ( Figure 8.2 ). Since the sebaceous gland is sterile, it follows that any significant photochemical damage to the gland itself requires an exogenous porphyrin (or a pro drug such as ALA). Any blue, red, or green color light source alone might result in P. acnes killing but would not be expected to cause significant sebaceous gland damage. Johnsson found that the extruded contents of the sebaceous follicle yielded a spectrum with an excitation peak ranging from 381–405 nm. Penetration arguments, of some wavelengths, not withstanding, this finding supports violet–blue light as an excellent color scheme for killing P. acnes .