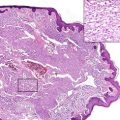
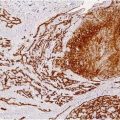
Fig. 37.1
Kaposiform hemangioendothelioma. Irregular tumor nodules growing in an infiltrative fashion and evoking a dense hyaline stromal response (Courtesy of H.Kutzner, Friedrichshafen)
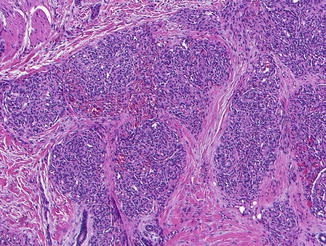
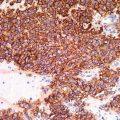
Fig. 37.2
Kaposiform hemangioendothelioma. Tumor nodules composed with well-canalized areas alternating with poorly canalized and solid-appearing areas resembling a capillary hemangioma (Courtesy of H.Kutzner, Friedrichshafen)
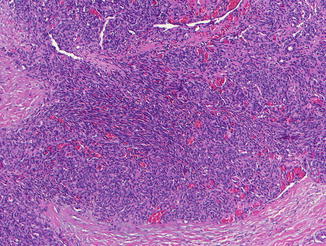
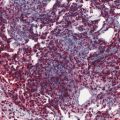
Fig. 37.3
Kaposiform hemangioendothelioma. Infiltrating sheets composed of variably spindled endothelial cells and slit-like vascular channels reminiscent of Kaposi sarcoma (Courtesy of H.Kutzner, Friedrichshafen)
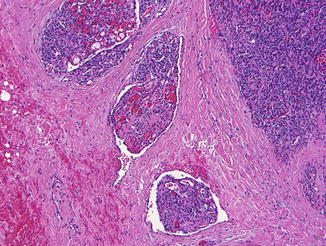
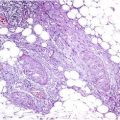
Fig. 37.4
Kaposiform hemangioendothelioma. Some areas show a glomeruloid pattern (Courtesy of H.Kutzner, Friedrichshafen)
Differential Diagnosis
The diagnosis is based upon the histology and on its correlation with clinical features, in particular the depth of the lesion. The relationship between KHE and tufted angioma is controversial. The “cannon ball” distribution of skin nodules and their “tufting” into ectatic spaces are characteristic of tufted angioma. In KHE, the tumor nodules coalesce, enlarge, and assume a widely infiltrative pattern within the fibroblastic stroma, a feature not observed in tufted angioma. A different pattern of expression of D2-40 has been reported as useful to distinguish the two entities. Nevertheless, the morphological overlap between KHE and tufted angioma has led to consider the two lesions into the same disease spectrum and that tufted angioma may represent a minor form of KHE.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


